
|Articles|November 21, 2012
2013 Radiology Coding Update: Focus on Head and Neck
Author(s)Whitney L. Jackson
In 2013, CMS will dramatically reduce the number of codes used for radiology, as well as how your services are coded.
Advertisement
For radiology groups and their coders, 2013 will be all about the head and neck, according to industry coding experts. CMS is set to implement changes on Jan. 1 that will not only dramatically reduce the number of codes used for radiology, but also how your services are coded.
Overall, the coding changes focus on three specific areas: cervical spine, nuclear medicine, and interventional radiology. The cervical spine code is currently classified as a low pay/high use code, and CMS is reviewing whether its value should be changed. In addition, the agency will release a new code structure for nuclear medicine next year.
The biggest impact on your bottom line, however, will be with the codes for interventional radiology, said Melody Mulaik, president and co-founder of Coding Strategies.
“CMS is deleting all the narrow interventional diagnostic imaging codes that exist and bundling them all together,” she said. “They’re following the trend that we’ve been seeing over the years of creating bundled codes that include catheter placement and diagnostic imaging.”
This step is a continuation of CMS’s move toward bundling more codes that routinely appear together. In this case, the agency will bundle several codes for services that you perform together at least 75 percent of the time. Several cervicocerebral angiography codes will now be bundled, as well as many transcatheter therapy infusion for thrombolysis and intravascular foreign body retrieval codes.
In December, the Radiology Business Management Association will hold a
It’s not yet clear how extensively these coding changes will impact your bottom line. But to avoid leaving any money on the table, Mulaik recommended you review your documentation procedures and how you communicate with your coders. Your coding staff must be properly educated about the coming coding changes to understand how improper coding will impact your practice. Mulaik suggested audio webinars or coding seminars as easily accessible ways to get pertinent information.
Radiologists in private practice, however, don’t worry Mulaik much. She is more concerned over the amount of reimbursement hospitals will likely lose due to ineffective charge capture models.
“A big problem facing radiology is that, currently, surgical codes that apply to interventional radiology cases conducted in a hospital are packaged, so hospitals haven’t paid much attention to them,” she said. “Now, they’re going to be responsible for revenue for the radiologist. That’s huge, and there’s the potential that hospitals don’t really understand the impact of this change.”
Consequently, she said, fluid communication between the technologist, interventional radiologist, and the hospital’s health information management staff will become vital to complete radiology reimbursement.
With this many coding changes, it can be a challenge to remain in compliance, according to Tara Conklin, a radiology coding analyst with CodeRyte. There are steps you can take, however, to make sure you’re following Medicare’s rules.
Mostly importantly, document your services clearly and consistently. For example, she said, always list exam titles and clinical indications separately from findings or impressions. Keep your descriptions brief and always include modality with the exam title.
In addition, make a concerted effort to play an active role in correctly coding for your services. Take the time to dictate a title even if you or your technologist have included one in the order. Doing so will ensure proper reimbursement.
“The physician is ultimately responsible for the codes submitted and the final documentation,” Conklin said. “Too often the dictated note does not match or clearly support the ordered exam title, forcing coders to make assumptions using incomplete data or take the time to pursue the physician for clarification.”
You can also avoid insufficient reimbursement and ensure compliance by including all required details for correct documentation. For example, she said, when coding for an obstetric ultrasound, be sure to note both the amniotic and gestational sacs. Documenting both parts is critical. If your notes are incomplete, you’ll be reimbursed for the lesser service. However, if you document only the higher-reimbursement service, you risk noncompliance edits or a rejected claim.
No matter the situation, Mulaik said, radiologists must make themselves as knowledgeable as possible about procedure codes and coding changes.
“It’s important for radiologists to be part of the conversation and identify any potential problems with coding,” she said. “The codes and the code definitions themselves really aren’t that confusing. It’s all about knowing what they are and making sure the documentation is sufficient.”
Advertisement
Related Content
Advertisement










Advertisement
Advertisement
Trending on Diagnostic Imaging
1
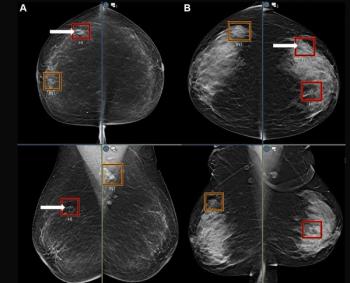
Mammography Study Suggests AI Can Bolster the Ability of General Radiologists to Detect Breast Cancer
2
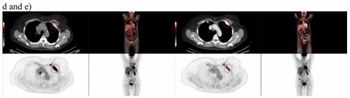
Study Suggests FDG-PET Better than CT for Assessing Treatment Response for Metastatic Breast Cancer
3
A Closer Look at the Evolution and Emerging Insights with Amyloid and Tau PET for Dementia and Alzheimer’s Disease
4
Could an Emerging Ultrasound Device Facilitate More Efficient Vascular Access Workflows?
5