
|Articles|December 1, 2007
Advances solve problems in imaging patients with AAA stents
Advanced imaging techniques are expanding the scope of investigation of patients undergoing stenting for acute aortic aneurysm. Dynamic 4D CT is giving interventional radiologists critical information about sporadic, and therefore difficult-to-detect, graft-related endoleaks that may be causing an aneurysm sac to enlarge after endovascular repair.
Advertisement
Advanced imaging techniques are expanding the scope of investigation of patients undergoing stenting for acute aortic aneurysm. Dynamic 4D CT is giving interventional radiologists critical information about sporadic, and therefore difficult-to-detect, graft-related endoleaks that may be causing an aneurysm sac to enlarge after endovascular repair.
Dynamic CT work coming out of the University of Utrecht in the Netherlands is showing that there is a 10% variation in the diameter of the thoracic aorta as blood passes through the circulation. This variation corresponds to changes of up to 3 mm in diameter during the cardiac cycle.
"You can imagine this would lead to intermittent endoleaks during the cardiac cycle in aneurysms that we treated. There are similar changes at the aortic neck in renal aneurysms, where we get up to 15% diameter changes before and after endovascular repair," said Dr. Richard G. McWilliams of Royal Liverpool Hospital in the U.K. at the 2007 annual meeting of the Cardiovascular and Interventional Radiology Society of Europe.
Computerized modeling of CT data may greatly simplify the planning and sizing of fenestrated stent-grafts to fit a specific aortic aneurysm, said Dr. Roy Greenberg of The Cleveland Clinic Foundation in the U.S. A computer program is using CT scans to create a mathematical model that reconstructs and calculates the intersections of the aortic surface to provide what amounts to a mechanical drawing that will allow interventional radiologists to select an appropriately sized fenestrated device.
"With a fenestrated graft, we start with axial imaging, but axial imaging can't tell us the whole story. You may have complex reconstructions and algorithms that give all sorts of distances, but the fundamental question you're asking is, Where is this aorta healthy?", Greenberg said. "The world is going to get a lot simpler [with a computer] program that selects the branch vessels. These are the types of technologies that will allow us to take planning and sizing of grafts to the next level."
Imaging is a particular problem when an aneurysm sac appears to be enlarging after endovascular repair. It not only must carefully calculate the sac diameters to confirm that there indeed has been an increase in size but must also attempt to determine whether the cause of the enlargement is endoleak, migration, attachment site dilatation, or movement at the modular connections.
An increase of 5 mm in sac diameter is the threshold generally agreed upon for considering an aneurysm to have enlarged after endovascular repair. Aneurysm measurements can vary greatly, however, depending on when and how the sac is evaluated. Baseline measurement should rely on the first CT scan taken after endovascular repair, rather than pretreatment scans. Findings on pretreatment scans may be misleading because they were done weeks or even months before interventional repair, McWilliams said.
The same axis should be chosen for each evaluation. An aneurysm may appear to be enlarging only because interpreters have chosen a different axis during follow-up. In one example, the same aneurysm could be measured at 7.1, 8, or 8.3 mm, depending on the axis.
Patients who have an aneurysm sac that may be increasing in size typically undergo a combination of ultrasound, radiograph, and CT studies. An arterial phase CT is routine for follow-up, but complex cases may require triple-pass CT or translumbar sac pressure measurement.
Microleaks associated with leakage from suture holes, alterations in polyester weave, or erosion where graft fabric abducts the edges of stent components may be manifested by small jets of color on Doppler ultrasound or small areas of enhancement adjacent to the graft on CT. These leaks may be detected by injecting by hand the distal lumen occlusion, McWilliams said.
An often forgotten area in aneurysm surveillance is the iliac zone, he said. In one case, a stent was not positioned perfectly at the bifurcation because the native iliac artery was running posteriorly, but the interventionalist had not tilted the stent caudally to the orientation of the common iliac artery, and therefore missed the proper location by 3 or 4 cm.
"If you don't engage the iliac and get a good overlap zone, then as the limb starts to dilate, you get contraction into the sac with rupture in some cases," he said.
Advertisement
Related Content
Advertisement












Advertisement
Advertisement
Trending on Diagnostic Imaging
1
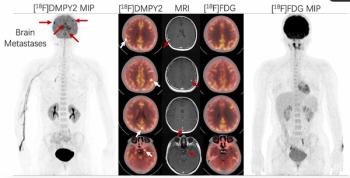
Emerging PET Radiotracer May Enhance Detection of Small Metastases in Patients with Advanced Melanoma
2
Can Biomechanical CT Have an Impact in Opportunistic Screening for Osteoporosis?
3
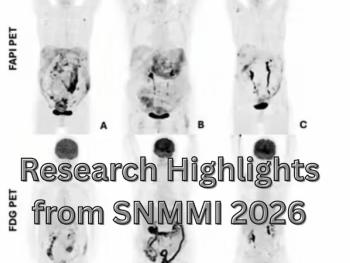
Molecular Imaging in Focus: Key Takeaways from the 2026 SNMMI Conference with Michael Hofman, MBBS, FRACP
4
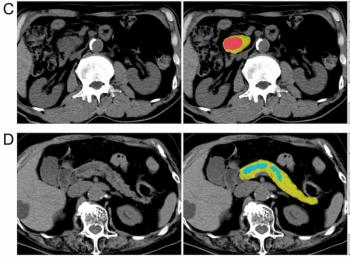
Can AI Enhance Non-Contrast and Contrast-Enhanced CT Detection of Pancreatic Cancer?
5