
|Articles|March 3, 2005
Cardiology PACS basics: The DICOM standard
Dr. Jonathan Elion is a cardiologist, computer scientist, and cofounder and chief medical officer of Heartlab, a company that develops systems for the digital management of cardiology reports and data sets. The former director of the cardiac image processing laboratory at the University of Kentucky, he has been involved in cardiac image processing since 1983.
Advertisement
Dr. Jonathan Elion is a cardiologist, computer scientist, and cofounder and chief medical officer of Heartlab, a company that develops systems for the digital management of cardiology reports and data sets. The former director of the cardiac image processing laboratory at the University of Kentucky, he has been involved in cardiac image processing since 1983.
Elion has had hands-on experience with electronic medical records, integration, HL7, and other technologies related to modern hospital information systems. He maintains an active practice in cardiology and is a fellow of the American College of Cardiology.
In an interview in February, Elion answered Diagnostic Imaging's questions about the role of DICOM in cardiology.
Q: What is DICOM?
The DICOM standard can trace its roots to 1983, when the American College of Radiology and the National Electrical Manufacturers Association began to create a standard method for the digital transmission of medical images. The resulting ACR-NEMA standard was first published in 1985 and later revised as version 2.0 in 1988. Version 3.0, published in 1993, was associated with a name change to Digital Imaging and Communications in Medicine.
DICOM specifies a standard network protocol for communications and defines information objects not only for images but also for patients, studies, reports, and other forms of related data. The goals of DICOM are to achieve compatibility and to improve workflow efficiency between imaging systems and other information systems in healthcare environments worldwide.
Every major diagnostic medical imaging vendor in the world has incorporated the standard into its product design, and most actively participate in the enhancement of the standard. Most of the professional societies throughout the world have supported and are participating in the enhancement of the standard as well.
Q: Describe your work on the DICOM committee.
My work with DICOM began in November 1992, as part of the initial group that met at the American College of Cardiology headquarters in Bethesda. Cardiologists, ACC staff, and representatives from industry discussed the challenge of interoperability of digital angiographic systems and decided to work on extending the DICOM standard to meet this need.
Led by Dr. Steven Nissen, we became Working Group 1 of the DICOM committee, addressing cardiac and vascular information. In 1995, we held our first demonstration at the ACC meeting in New Orleans, with 29 vendors using the reference software that I wrote and put into the public domain. It created and read angiographic and echocardiographic images in the newly extended DICOM standard format.
In 2001, I developed the software and reference data set for a similar demonstration showing the exchange of nonimage data using DICOM's structured reporting capabilities. I have been the cochair of DICOM Working Group 1 since 2000.
Q: Why is DICOM important for cardiology?
DICOM provides a standardized format for the exchange of cardiac images and information. It is the mechanism by which cath and echo images can be stored and shared not only within a hospital enterprise, but also to outreach facilities, physicians' practices, and even to one's home. The same applies to images from intravascular ultrasound, CT, and MR, as well as hemodynamic waveforms.
DICOM has to date played no significant clinical role in electrocardiography, although other standards do exist that cover this area. A very exciting development that should play out over the next 12 months is the ability of echo carts to transmit the measurements made by the sonographer using structured reporting portions of the DICOM standard.
Q: The DICOM standard has been adopted by a number of specialties, for example, radiology and ophthalmology. What unique challenges does cardiology bring to DICOM?
DICOM is used or will soon be used by cardiology, dentistry, endoscopy, mammography, ophthalmology, orthopedics, pathology, pediatrics, radiation therapy, radiology, and surgery. Cardiology introduces the challenge of moving images that, while not unique to cardiology, certainly are emphasized and required more than in most other disciplines.
The multimodality nature of cardiology also introduces the challenge of synchronizing information from several different sources, such as audio with echo images, and ECG waveforms with x-ray angiography. The nonimaging data involved in a cardiac study also tend to be far more comprehensive than the simple image and numeric reports that form the foundation of basic radiology systems.
Q: How is the DICOM standard developed and kept up to date? Please use an example from cardiology to illustrate the process.
The DICOM standards organization is administered by the NEMA diagnostic imaging and therapy systems division. Currently, 23 working groups of the DICOM committee perform most of the work on extending the standard and keeping it up to date.
The working groups submit their work as supplements to the Base Standards Working Group (WG-06), for its review, thereby helping to assure a degree of uniformity and coordination across all of the activities. Supplements to the standard are then published for public comment, followed by a formal voting process by DICOM members.
Some recent examples of supplements related to cardiology have completed this process:
- Supplement 72: Structured Reporting for Echocardiography
- Supplement 76: Structured Reporting for Quantitative Arteriography and Ventriculography
- Supplement 80: DVD-R as the interchange media for cardiology
Q: How widely accepted is DICOM among cardiology PACS vendors?
DICOM has been nearly universally accepted and adapted for cardiac imaging. It is starting to see significant progress with respect to the conveyance of other information like the echo measurements I mentioned. All current x-ray angiographic systems provide DICOM capabilities, and the small percentage of legacy systems installed before DICOM was available can be upgraded with after-market systems to provide DICOM output.
Most echo carts have a DICOM option, and again, there are after-market upgrades available either from the original manufacturer or from third parties that can provide DICOM capabilities. One exception, unfortunately, is 4D echocardiography (motion 3D images). DICOM standards to specify the interchange of these images are still making their way through the approval process, and, in the interim, several proprietary formats have emerged. This severely hampers interoperability and puts the physician at risk of being held hostage by echo cart manufacturers who are reluctant to make the format of the data available to customers or to PACS workstation providers.
Q: Where can cardiologists go for more information about DICOM?
The
Advertisement
Related Content
Advertisement













Advertisement
Advertisement
Trending on Diagnostic Imaging
1
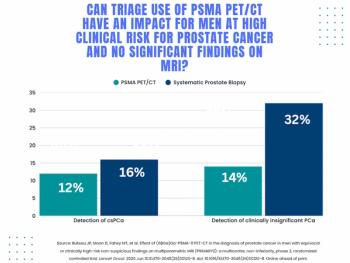
Study: PSMA PET/CT Reduces Biopsy Rate by Nearly 50 Percent for Men with Equivocal or Non-Suspicious Prostate mpMRI
2
Mammography Study: Can AI Detect Potential Breast Cancer Up to a Decade Prior to Diagnosis?
3
The Hidden Social Price of Remote Work in Radiology
4
Addressing Challenges in Radiology Reporting
5