

|Articles|May 1, 2007
Computer-aided diagnosis moves from breast to other systems
Author(s)Kunio Doi, PhD
Computer-aided diagnosis has become a part of routine clinical work for detection of breast cancer on mammograms.1-7 It is beginning to be applied in the detection and differential diagnosis of many different kinds of abnormalities in medical images obtained with various modalities.
Advertisement
Computer-aided diagnosis has become a part of routine clinical work for detection of breast cancer on mammograms.1-7 It is beginning to be applied in the detection and differential diagnosis of many different kinds of abnormalities in medical images obtained with various modalities. It has, in fact, become one of the major research subjects in medical imaging and diagnostic radiology.7-17 From 2003 to 2006, about 200 papers related to its use were presented at each of the RSNA annual meetings.
The initial phase of practical CAD use in clinical applications consisted of screening examinations for detection of cancer in the breast,1-7 lung,8,9,13 and colon.10 Commercial CAD systems for detection of these cancers are now available for clinical use.
Investigators1-6 have reported results from prospective studies on large numbers of screening mammography subjects, ranging from 8682 to 115,571, regarding the effect of CAD on the detection rate of breast cancer. All of these studies indicated an increase in the detection rates of breast cancer with use of CAD, though the results showed a large variation, from 1.7% to 26%, in this increase.
Areas of current CAD research include the chest, breast, colon, brain, liver, kidney, and skeletal and vascular systems. Three examples of CAD schemes being developed illustrate new approaches to practical clinical use.
In bone scintigraphy, it is time-consuming to identify multiple lesions such as bone metastases of prostate and breast cancers. Detecting subtle interval changes between two successive abnormal bone scans is difficult, because of variations in patient conditions, radioisotope accumulations, and the image quality of gamma cameras.
Figure 1 illustrates a temporal subtraction image obtained from a CAD scheme18 for detection of interval changes in successive whole-body bone scans. The sensitivity in the detection of interval changes, including both hot and cold lesions, was 95.3%, with 5.97 false positives per view. This CAD application was useful in assisting radiologists, providing an increase in detection accuracy and also a 30% reduction in reading time,19 similar to findings from use of temporal subtraction images obtained from chest radiographs.20 The clinical utility of this CAD scheme is being evaluated in a prospective study.
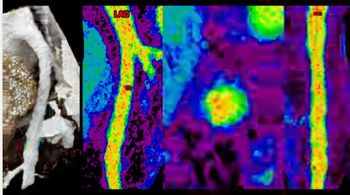
In the detection of intracranial aneurysms in CT and MR angiography, it is difficult and time-consuming for radiologists to find small and even medium-sized aneurysms, because of overlap with adjacent vessels and/or unusual locations. A CAD scheme21,22 was developed for automated detection of unruptured intracranial aneurysms in MRA (Figure 2). The sensitivity in detecting intracranial aneurysms ranging from 1 mm to 23 mm was 96%, with 3.2 false positives per patient. An observer study indicated use of the computer output improved radiologists' detection of intracranial aneurysms in MRA.23
Vertebral fracture or deformity is a common outcome of osteoporosis. Early detection of vertebral fracture is important because timely pharmacologic intervention can reduce the risk of subsequent additional fractures. Vertebral fractures can be visible on lateral chest radiographs, but investigators have noted that about 50% of such fractures visible on radiographs were underdiagnosed or underreported, even when they were severe. A CAD scheme24 was developed for detection of vertebral fractures on lateral chest radiographs to assist in radiologists' image interpretation and thus in the early diagnosis of osteoporosis (Figure 3). The sensitivity for detection of fracture cases was 95%, with 1.03 false positives per image, which resulted in an improvement in radiologists' detection performance.
PROBLEMS AND ISSUES
A large number of clinical cases with lesions must be used as the gold standard to develop a computerized scheme for CAD. Databases with adequate numbers of cases are usually not available to researchers, however. Establishing a gold standard is very difficult for most abnormalities in clinical images except in some limited situations where pathologic and/or other proofs are available.
It is therefore common to use the consensus of experts as a gold standard, although the variation in experts' judgments can be considerable. Disagreement between two radiologists in identifying small lung nodules in CT images, for example, was about 30%. Thus, it has been difficult for investigators to initiate research and development of new CAD schemes.
Once a reliable CAD scheme has been developed for a commercial product, it is necessary to obtain FDA approval for clinical use. This process has often been difficult for small companies because of the requirement of clinical studies for premarket approval instead of 510k.
Reimbursement is another important issue for the use of CAD in clinical studies. One reason mammographic CAD is now used widely is the reimbursement allowed for it. The sooner the reimbursement for other CAD schemes can be established, the greater the benefits will be from various CAD schemes for patient care.
It is likely that many CAD schemes will be assembled as packages and implemented as a part of PACS.13,15 The package for chest CAD, for example, may include computerized detection of lung nodules, interstitial opacities, cardiomegaly, vertebral fractures, and interval changes in chest images as well as computerized classification of benign and malignant nodules and the differential diagnosis of interstitial lung diseases. All chest images taken for any purpose will be subjected to a computerized search for the many different types of abnormalities included in the CAD package. Thus, potential sites of lesions, together with relevant information such as the probability of a certain disease, may be displayed on the workstation.
At present, most images in PACS are not being used for clinical purposes, except when current images of a patient are compared with previous ones of that patient. The vast majority of these unused images in PACS are currently "sleeping."17 Providing a set of benign and malignant images, or a set of images with known pathology that are similar to an unknown new case in question, would be useful in assisting radiologists in their differential diagnosis. If the new case were considered similar to one or more benign (or malignant) images by a radiologist, he or she would be more confident in deciding that the new case was benign (or malignant). It would be possible to search for and retrieve similar cases with similar images from PACS, if a reliable and useful method were developed for quantifying the similarity of a pair of images (or lesions) for visual comparison by radiologists.
Recent studies have indicated that the similarity of a pair of lung nodules in CT25 and of lesions in mammograms26,27 may be quantified by a psychophysical measure using an artificial neural network that is trained with the corresponding image features and subjective ratings given by a group of radiologists.
CAD is still in the infancy of its full potential for applications to many different types of lesions obtained with various modalities.16 It is likely that CAD will become a standard of care for diagnostic examinations in daily clinical work.
Dr. Doi is Ralph W. Gerard professor in the biological sciences and director of the Kurt Rossmann Laboratories for Radiologic Image Research in the radiology department at the University of Chicago. He is a shareholder of Hologic (R2 Technology). CAD technologies developed in the Rossmann laboratory have been licensed to R2 Technology, Deus Technology, Riverain Medical Group, Mitsubishi Space Software, Median Technologies, GE, and Toshiba.
References
- Freer TW, Ulissey MJ. Screening mammography with computer-aided detection: prospective study of 12,860 patients in a community breast center. Radiology 2001;220:781-786.
- Gur D, Sumkin JH, Rockette HE, et al. Changes in breast cancer detection and mammography recall rate after the introduction of a computer-aided detection system. J Natl Cancer Inst 2004;96:185-190.
- Birdwell RL, Bandodkar P, Ikeda DM. Computer-aided detection with screening mammography in a university hospital setting. Radiology 2005;236:451-457.
- Cupples TE, Cunningham JE, Reynolds JC. Impact of computer-aided detection in a regional screening mammography program. AJR 2005;185:944-950.
- Morton MJ, Whaley DH, Brandt KR, Amrami KK. Screening mammograms: interpretation with computer-aided detection-prospective evaluation. Radiology 2006;239:375-383.
- Dean JC, Ilvento CC. Improved cancer detection using computer-aided detection with diagnostic and screening mammography: prospective study of 104 cancers. AJR 2006;187:20-28.
- Giger ML. Computerized analysis of images in the detection and diagnosis of breast cancer. Semin Ultrasound CT MR 2004;25:411-418.
- Abe H, MacMahon H, Shiraishi J,et al. Computer-aided diagnosis in chest radiography. Semin Ultrasound CT MR 2004;25:432-437.
- Li Q, Li F, Armato SG III, et al. Computer-aided diagnosis in thoracic CT. Semin Ultrasound CT MR 2005;26:357-363.
- Yoshida H, Dachman AH. Computer-aided diagnosis for CT colonography. Semin Ultrasound CT MR 2004;25:404-410.
- Doi K, MacMahon H, Giger ML, Hoffmann KR, eds. Computer aided diagnosis in medical imaging. Amsterdam: Elsevier, 1999:3-560.
- Doi K, MacMahon H, Katsuragawa S, et al. Computer-aided diagnosis in radiology: potential and pitfalls. Eur J Radiol 1999;31:97-109.
- Doi K. Computer-aided diagnosis in digital chest radiography. Advances in digital radiography: RSNA categorical course in diagnostic radiology physics. 2003:227-236.
- Doi K. Overview on research and development of computer-aided diagnostic schemes. Semin Ultrasound CT MR 2004;25:404-410.
- Doi K. Current status and future potential of computer-aided diagnosis in medical imaging. Br J Radiol, Special Issue 2005;78:S3-S19.
- Doi K. Diagnostic imaging over the last 50 years: Research and development in medical imaging science and technology. Phys Med Biol 2006;51:R5-R27.
- Doi K. Computer-aided diagnosis in medical imaging: historical review, current status and future potential. J Comput Med Imaging Graphics 2007, Special Issue on Computer-aided diagnosis (CAD) and image-guided decision support (in press), doi:10.1016/j.compmedimg.2007.02.002
- Shiraishi J, Li Q, Appelbaum D, et al. Development of a computer-aided diagnostic scheme for detection of interval changes in successive whole-body scans. Med Phys 2006;34:25-36.
- Shiraishi J, Appelbaum D, Pu Y, et al. Usefulness of temporal subtraction images for detection of interval changes in successive whole-body bone scans: JAFROC analysis of radiologists' performance. Presented at the Annual Meeting of the RSNA 2006, Nov. 25 to Dec. 1, 2006, Chicago, page 373, Scientific Program book.
- Kakeda S, Kamada K, Hatakeyama Y, et al. Effect of temporal subtraction of technique on reading time and diagnostic accuracy in the interpretation of chest radiographs. AJR 2006;187:1253-1259.
- Arimura H, Li Q, Korogi Y, et al. Automated computerized scheme for detection of unruptured intracranial aneurysms in three-dimensional MRA. Acad Radiol 2004;11:1093-1104.
- Arimura H, Li Q, Korogi Y, et al. Computerized detection of intracranial aneurysms for 3D MR angiography: Feature extraction of small protrusions based on a shape-based difference image technique. Med Phys 2006;33:394-401.
- Hirai T, Korogi Y, Arimura H, et al. Intracranial aneurysms at MR angiography: Effect of computer-aided diagnosis on radiologists' detection performance. Radiology 2005;237:605-610.
- Kasai S, Li F, Shiraishi J, et al. Computerized detection of vertebral compression fractures on lateral chest radiographs: Preliminary results of a tool for early detection of osteoporosis. Med Phys 2006;33:4664-4676.
- Li Q, Li F, Shiraishi J, et al. Investigation of new psychophysical measures for evaluation of similar images on thoracic CT for distinction between benign and malignant nodules. Med Phys 2003;30:2584-2593.
- Muramatsu C, Li Q, Suzuki K, et al. Investigation of psychophysical measure for evaluation of similar images for mammographic masses: Preliminary results. Med Phys 2005;32:2295-2304.
- Muramatsu C, Li Q, Schmidt RA, Suzuki K, et al. Experimental determination of subjective similarity for pairs of clustered microcalcifications on mammograms: Observer study results. Med Phys 2006;33:3460-3468.
Advertisement
Related Content
Advertisement












Advertisement
Advertisement
Trending on Diagnostic Imaging
1
SCCT: Should Photon-Counting CT Be the New Standard for Assessing CAD Prior to TAVR?
2
FDA Clears AI-Enabled Ultrasound for High-Volume Clinical Settings
3
AI in Radiology: Emerging Trends, Current Obstacles and Future Directions
4
Diagnostic Imaging's Weekly Scan: July 5 — July 11
5