
|Articles|April 1, 2009
CT and MRI show complexparanasal sinus anatomy
Inflammation of the upper airways is most often due to the common cold. CT and MRI show complexparanasal sinus anatomy.
Advertisement
Inflammation of the upper airways is most often due to viral infectious rhinitis, that is, the common cold. If the rhinitis has superimposed on a bacterial infection, this may lead to rhinosinusitis. Although either can cause inflammation, the upper airways are infrequently affected by primary tumors of the nasal cavity or destructive inflammatory disorders such as Wegener's granulomatosis.
Rhinosinusitis affects the quality of life of almost 25% of the U.S. adult population.1 Previously known as sinusitis, it is now known as rhinosinusitis because acute rhinosinusitis is most commonly preceded by acute or chronic rhinitis and is likely to occur when there is a disturbance in the mucus drainage system with subsequent nasal airway inflammation.
People with diabetes, immunocompromized patients, and individuals with congenital abnormalities, cystic fibrosis, or Kartagener's syndrome (cilia dysfunction syndrome) are particularly prone to chronic fungal sinusitis.2 Chronic rhinosinusitis is due to infection in the majority of cases, notably the coagulase positive and negative species of Staphylococcus.
Mucus membrane covered with stratified nonkeratinized squamus epithelium lines the nose posterior to the vestibule. The remainder of the nasal cavity, except the roof, is lined with pseudostratified ciliated columnar epithelium and goblet cells that produce the nasal mucus.3 One function of nasal mucus is to capture inhaled particles. The mucus blanket is then transported along specific pathways by the coordinated wave motion of cilia lining the nasal cavity, beating toward the nasopharynx.
The mucus consists of two layers that are functionally distinct but structurally continuous. The periciliary fluid is a lubricating layer in which the cilia beat. The viscous layer, which lies above, traps particulate matter.4 The ciliary transport system moves mucus within the upper and lower respiratory tracts toward their natural ostium, bypassing obstructions on the mucosal surface.5 Disturbance in the nasal mucociliary clearance of the mucus blanket leads to sinusitis.
Rhinosinusitis is diagnosed primarily by clinical history and endoscopic examination. Antibiotics are prescribed for acute sinusitis and chronic rhinosinusitis to prevent disease progression. Antihistamines and topical anti-inflammatory agents (corticosteroids) are useful in patients whose sinusitis has an allergic component. Corticosteroids are not, however, beneficial in acute infec tious sinusitis.
Ancillary medical treatment should be attempted to help relieve acute episodes of mucosal edema. Preoperative imaging should not be performed during episodes of acute exacerbation because simple mucus and edema can mimic mucosal swelling, polyps, and retention cysts.
Surgery may be considered if the above medical therapies are unsuccessful. Chronic rhinosinusitis was traditionally treated with radical procedures, including the Caldwell-Luc operation (open maxillary sinus surgery), external ethmoidectomy (ethmoid sinus surgery), and external frontoethmoidectomy, sublabial, and trans-septal septoplasty for the sphenoid sinus.6 These procedures carry the risk of potentially serious neurological and vascular complications, such as optic nerve damage and internal carotid artery transection. This is particularly the case for sphenoid sinus surgery. Paresthesia of a dermatome is a more frequent complication. In the Caldwell-Luc procedure, for example, the infraorbital nerve is most likely to be affected.
The development of functional endoscopic sinus surgery (FESS) means that chronic rhinosinusitis can now be alleviated using minimally invasive techniques. Extensive removal of diseased mucosa is discouraged following improved understanding of the mucociliary system. The mucoperiosteum is not stripped during FESS, as it is with radical surgery. The health of the frontal and maxillary sinuses is now thought to be dependent on the anterior ethmoid complex.7,8
FESS can be performed under local or general anesthetic. The aim is to enlarge the natural sinus ostia, preserving and restoring the normal physiological systems of mucociliary drainage and ventilation. The use of FESS has coincided with a dramatic increase in preoperative imaging. Imaging has become an essential prerequisite to planning interventions for inflammatory disorders of the paranasal sinuses.
DESCRIPTIVE TERMS
The reporting of paranasal sinus anatomical nomenclature has been influenced by the approach suggested by the U.S.-based International Anatomic Terminology group.9 Adoption of precise descriptive terminology narrows the scope for misinterpretation.
The adult human nasal cavity is formed by lateral and medial walls and the cavity's roof and floor. The floor is formed by the palatine process of the maxilla anteriorly and the horizontal plate of the palatine bone posteriorly. The most anterior aspect of the roof is the nasal cartilage and a small portion of the nasal and frontal bone. Lateral to the cribriform plate is the ethmoid fovea, and together they form the roof; they also form part of the floor of the anterior cranial fossa.
The nasal septum forms the medial wall. The septal cartilage and ethmoid perpendicular plate lie anteriorly. The vomer is located inferoposteriorly. Superiorly, the vomer articulates with the body of sphenoid, while its free posterior edge leads to the nasopharynx. The lateral wall is formed by the nasal bone anterosuperiorly and by the maxilla, a small portion of lacrimal bone (housing the lacrimal duct), the ethmoid bone, inferior concha bone, and the palatine bone posteriorly.
The lateral wall has three projections: the superior, middle, and inferior turbinates. The superior and middle turbinates are formed from the ethmoid bone complex, while the inferior turbinate is the inferior concha bone. The space below each turbinate is defined as the meatus. The frontal, anterior ethmoid, and maxillary sinuses drain through the hiatus semilunaris to exit through the middle meatus. The posterior ethmoid complex and sphenoid sinus drain into the sphenoethmoid recess and exit via the superior meatus.10 Isolated disease is more commonly found in the anterior ethmoid complex and its related structures than in the posterior ethmoid complex and its related structures.11
The ethmoid complex, the ostiomeatal complex (OMC), and the lateral nasal wall are central to paranasal anatomy and inflammatory disease. The ostiomeatal complex is the final point in the drainage pathway of the maxillary, anterior ethmoid, and frontal sinuses.12 It consists of the maxillary sinus ostium, ethmoid infundibulum, frontoethmoidal recess (alternatively, the frontonasal recess), uncinate process (anatomical variation can obstruct the OMC), middle turbinate, and middle meatus.10
The middle turbinate, which is part of the ethmoid complex, is a bony structure with a vertical and a horizontal attachment. The anterior third inserts vertically onto the lateral end of the cribriform plate, and the middle third turns laterally toward the lamina papyracea, where it turns inferiorly. The most posterior third becomes horizontal and inserts laterally onto the lamina papyracea (Figure 1). The International Anatomic Terminology group defines the vertical and horizontal portions of the middle turbinate as the “basal lamella of the middle turbinate.”9
The middle turbinate may be pneumatized, but it is not involved in the mucociliary transport system. The basal lamella of the middle turbinate is a border between the anterior and posterior groups of ethmoid cells. The anterior and posterior ethmoid complexes are anatomically and physiologically distinct categories according to definition, patterns of mucociliary secretion, transport, and embryological development.
The frontal sinuses, which are paired, are normally asymmetrical with bony septae (usually incomplete). The frontal sinuses lie between the inner and outer table of the frontal bone, draining via the frontoethmoidal recess into the middle meatus. They can be hypoplastic, hyperplastic, or aplastic. The frontoethmoidal recess can be obstructed anteroinferiorly by enlarged agger nasi cells or posteriorly by enlarged ethmoid bullae.
The maxillary sinuses are the largest of the paranasal sinuses and are pyramidal in shape. The medial wall forms the base, and the apex points toward the zygoma. The roof is the orbital floor, which is grooved by the infraorbital canal and neurovascular bundle. The thin bone housing the infraorbital canal can be affected by reactive osteitis secondary to chronic inflammatory sinus disease. The alveolar plate of the palatine bone forms the floor.
The lateral nasal wall is the medial wall of the maxillary sinus. Its small defects, which are accessory maxillary sinus ostia, should not be mistaken for bony erosions. The posterior wall narrows and forms the anterior boundary of the pterygopalatine fossa. The pterygopalatine fossa is an important pathway in the dissemination of infection or intracranial tumor spread. It communicates with the orbit, nasopharynx, paranasal sinuses, infratemporal fossa, and middle cranial fossa.
The maxillary sinus ostium lies in the superomedial aspect of the medial sinus wall, at the lateral end of the ethmoid infundibulum (Figure 2). The ethmoid infundibulum drains through the semilunar hiatus and finally into the middle meatus. The sphenoid sinus, which is symmetrical, lies within the sphenoid bone and varies in size. The pituitary fossa and gland are superior, while the nasopharynx and the eustachian tubes and cushions are inferior. The cavernous sinuses are at the lateral end, and the clivus lies posteriorly.
The intracavernous portion of the internal carotid artery courses superiorly along the body of the sphenoid sinus. If the ICA lies within the lumen of the sphenoid sinus, this should be flagged. Surgeons find the most posterior ethmoid cell and break through it to enter the sphenoid sinus. If it is a sphenoidethmoid cell, the ICA and optic nerve can be damaged. The sphenoid sinus drains through a small ostium in the anterior wall, close to its roof, into the sphenoethmoid recess (Figure 3).
A study of 100 patients with chronic sinusitis and no previous surgical intervention found that disease involvement was most common in the middle meatus, followed by the middle meatus with associated maxillary sinus, frontal sinus, posterior ethmoid complex, and sphenoid sinus.13
ANATOMICAL VARIANTS
Surgeons should be made aware of a number of anatomical variants if these are observed on imaging. In the anterior ethmoid complex, the Haller cell (infraorbital cell) can lie anywhere along the surface of the infraorbital floor. These cells are significant if they are enlarged or situated near or at the ostiomeatal complex. A narrowed ethmoid infundibulum or maxillary sinus ostium will disrupt the normal physiological drainage and ventilation.
Sphenoethmoid cells are the most posterior ethmoid cells to become pneumatized. Known as ONDI (U.S.) or ONODI (Europe) cells, they extend laterally and, to a certain degree, superiorly. Posterolateral extension may expose the optic nerve and the ICA. This is clinically significant because locating the sphenoid sinus involves direct puncture through the last cell of the ethmoid complex. If the sphenoethmoid cell has extended posterolaterally, the nerve and artery may be damaged, with disastrous consequences.
The ethmoid roof, another significant posterior structure, is classified into three Keros categories. The olfactory bulb lies on the cribriform plate. The ethmoid fovealis is laterally attached to the cribriform plate, and its configuration is variable. The olfactory fossa is 1 to 3 mm deep with a short lateral lamella of the cribriform plate in Keros type I. In type II, the olfactory fossa is 4 to 7 mm deep, and in type III, it is 8 to 16 mm deep with a long lateral lamella. Type III is the most significant when considering surgery because it is vulnerable to damage. Asymmetry of the ethmoid roof is also surgically relevant in order to avoid skull base injury.9
OPTIMUM IMAGING
CT is now the primary imaging modality for pre- and postendoscopic assessment of acute and chronic rhinosinusitis. CT images provide an excellent road map for the endoscopist, delineating the bony anatomy, any anatomical variants, and the extent of sinomucosal disease. CT is the preferred modality for the assessment of disease severity. Particular attention should be paid to the cribriform plate, fovea ethmoidalis, lamina papyracea, and the basal lamella of the middle turbinate when checking for postoperative complications.
MRI is reserved for the evaluation of complicated sinusitis, any intracranial and orbital complications, cerebrospinal fluid leaks, subperiosteal abscesses, epidural or subdural empyema, or lateral extension into the orbits from the frontal sinuses. It is superior in differentiating inflammatory conditions from neoplastic processes. Abscesses can be differentiated from tumor using postcontrast fat-saturated T1-weighted imaging or diffusion-weighted MRI. T2-weighted contrast-enhanced sequences show subtle extradural disease. 14 MRI is also more sensitive than CT in differentiating neoplastic tissue from vasogenic edema, detecting intracranial and perineural spread, and identifying any cartilagenous invasion.15
Radiologists need to be aware of the normal nasal mucosal cycle. Changes to nasal mucosal volume occur cyclically, alternating from side to side.14 This should not be interpreted as pathology. Cyclical changes affect the turbinate mucosa, nasal septum, lateral wall and cavity floor, nasolacrimal ducts, and ethmoid sinuses. The frontal, maxillary, and sphenoidal sinuses are not affected. 16 Normal mucosa in areas affected by a cyclical change is isointense on T1- weighted MRI and shows increased signal on T2-weighted imaging.10 Researchers have suggested that paranasal mucosal thickening of 3 mm or less seen on MRI is not clinically significant and is common in asymptomatic patients.10 MRI signal variation in the sinonasal secretions can occur due to differences in the inherent properties of the secretions or extrinsic additional components such as hemorrhage.12
Axial CT data sets can now undergo multiplanar reformatting, thanks to improvements in software. Surgeons generally prefer to see coronal images because these resemble the endoscopic view.13-15,17 Coronal images are also believed to provide finer osseous lamellae detail than axial images, if both sets of images can be acquired problem free.
Coronal CT imaging was previously performed with the patient lying prone with the neck hyperextended. Images were acquired in contiguous sections of 3 to 5 mm/sec, with variable table-feed speeds of 2 to 3 mm/sec.16 Hyperextension is particularly difficult and uncomfortable for elderly patients, however, leading to motion artifacts. The presence of mercury-based dental fillings can also lead to suboptimal images.
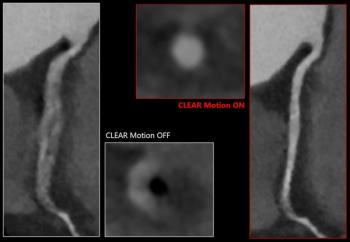
Good-quality reformatted coronal images can be acquired from four- and 16-slice CT scanners. Commercially available 32-, 40-, and 64-slice CT units that operate with faster scanning times, 0.1-mm slice thickness, and no gantry tilt have reduced the likelihood of motion artifacts. Patients can also be imaged supine, which is more comfortable and further lessens the chance of movement. Artifacts from dental amalgam are still a problem, though.16,18 The trade-off for this improvement is an increase in radiation dose, due to the increase in peak kV required to improve resolution and decrease scanning time.16 Low-dose techniques can counter this disadvantage (Figure 4).
We perform paranasal sinus imaging on 16- and 32-slice CT units. Patients lie supine with the head neutral and are not required to take decongestants prior to imaging. Axial slices are acquired at 1 mm (16-slice) and 0.5-mm (32-slice) intervals, with sections parallel to the orbitomeatal line or parallel to the hard palate. Data sets are reconstructed with 1-mm slice thickness at 2 to 5-mm intervals in the coronal and sagittal planes. The mAs is kept to a minimum (40 mAs) to reduce dose.
The wide individual variability of what is normal and the common occurrence of anatomical variants make it particularly important to understand sinus anatomy well. Comprehensive anatomical knowledge has implications for defining disease extent, identifying important surgical landmarks, identifying surgically relevant structures, and understanding postsurgical changes.
The prospect of smaller portable scanning units in outpatient or intraoperative settings in future is exciting. Meanwhile 64- and 256-slice CT scanners promise to provide exquisite bony detail in a very short time. The importance of radiation protection and the need for low-dose protocols should not be forgotten, though.
Advertisement
Related Content
Advertisement












Advertisement
Advertisement
Trending on Diagnostic Imaging
1
AI in Radiology: Emerging Trends, Current Obstacles and Future Directions
2
Canon Medical Unveils Advances in AI-Enabled CT Software
3
FDA Clears AI-Enabled Ultrasound for High-Volume Clinical Settings
4
Study Says Use of 18F-flotufolastat PET/MRI May Reduce Prostate Biopsies by More Than 50 Percent
5