
|Articles|April 23, 2007
CT colonography bests conventional screening in cost-effectiveness test
Author(s)Pia Pyne Miller
A new study has found that virtual colonoscopy with the removal of lesions 6 mm or greater is more cost-effective and just as clinically effective as optical colonoscopy or flexible sigmoidoscopy that targets polyps regardless of size.
Advertisement
A new study has found that virtual colonoscopy with the removal of lesions 6 mm or greater is more cost-effective and just as clinically effective as optical colonoscopy or flexible sigmoidoscopy that targets polyps regardless of size.
The cost-benefit analysis, involving 100,000 persons over 50 years old, determined that targeting lesions of less than 5 mm with optical colonoscopy and flexible sigmoidoscopy yields little additional diagnostic information to justify the cost. These approaches fell short of CT virtual colonoscopy with the removal of 6 mm or larger lesions for the estimated value per life-year gained and for avoiding complications.
Dr. Perry Pickhardt, an associate professor of radiology at the University of Wisconsin, and Dr. Cesare Hassan, a gastroenterologist in Rome, collaborated on the analysis. It will be published in the June 1 issue of Cancer, a journal of the American Cancer Society.
Effective screening through increased use of any of several available tests is considered a key to reducing deaths from colorectal cancer, the third most common cause of cancer death among both men and women in the U.S. Despite the availability of effective screening tests, screening rates remain low and deaths related to colorectal cancer remain high, Pickhardt and Hassan said in a release.
Their findings contradict previous published research showing that optical colonoscopy and flexible sigmoidoscopy of all sizes of polyps are more cost-effective than virtual CT-based colonoscopy. However, those studies ignored current guidelines for CT colonoscopy recommending reporting only polyps greater than 5 mm, Pickhardt and Hassan said.
By following that recommendation, Pickhardt and Hassan found that CT colonoscopy with optical colonoscopy follow-up for polyps larger than 5 mm was the most cost-effective screening test. The cost of life-year gained from virtual CT screening with a 6-mm threshold for follow-up was $4361 compared with $9180 for optical colonoscopy. For virtual CT screening with no polyp size threshold the cost per life-year gained was $7138, compared with $7407 for flexible sigmoidoscopy.
The incremental costs of working up lesions smaller than 6 mm uncovered with virtual CT screening were $118,440 per additional life-year gained. Moreover, working up these small, almost always benign polyps with optical colonoscopy caused considerable complications, Pickhardt and Hassan said. The study found almost half of all complications from optical colonoscopy were attributed to the workup of small lesions.
Targeting small lesions did not improve screening efficacy and reduced colorectal cancer incidence by only 1.3%, they said.
Virtual CT colonoscopy may also help reduce public objections to the traditional invasive approaches to colorectal screening and increase compliance with recommended screening guidelines, Pickhardt and Hassan said.
For more information from the Diagnostic Imaging archives:
Advertisement
Related Content
Advertisement













Advertisement
Advertisement
Trending on Diagnostic Imaging
1
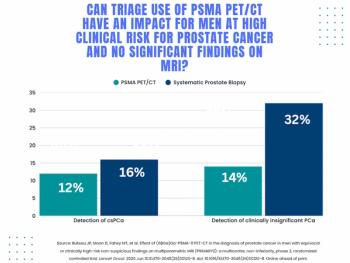
Study: PSMA PET/CT Reduces Biopsy Rate by Nearly 50 Percent for Men with Equivocal or Non-Suspicious Prostate mpMRI
2
Addressing Challenges in Radiology Reporting
3
The Hidden Social Price of Remote Work in Radiology
4
Mammography Study: Can AI Detect Potential Breast Cancer Up to a Decade Prior to Diagnosis?
5