

|Articles|December 18, 2008
Desmoteplase trial disappoints despite novel use of imaging
Author(s)NeedsFixing
Despite encouraging earlier results, the much-awaited follow-up phase III DIAS-2 trial did not show any improvement in clinical response at 90 days for ischemic stroke patients who were given either of two doses of desmoteplase up to nine hours after the onset of symptoms of stroke compared with those who were given placebo.
Advertisement
Despite encouraging earlier results, the much-awaited follow-up phase III DIAS-2 trial did not show any improvement in clinical response at 90 days for ischemic stroke patients who were given either of two doses of desmoteplase up to nine hours after the onset of symptoms of stroke compared with those who were given placebo.
The clot-busting drug tissue plasminogen activator (tPA), the only recommended treatment for acute ischemic stroke, is approved for use within three hours of the onset of symptoms. In previous investigational trials (DIAS-1 and DEDAS2), a new drug, desmoteplase, which is derived from vampire bat saliva, was shown to have a highly specific action and to be safe and effective over a longer treatment window than tPA. Efficacy in these trials was measured as the amount of reperfusion -- restoration of blood flow -- and the clinical outcome at three months for patients who were judged most likely to benefit from treatment.
Dr. Werner Hacke, of the University of Heidelberg in Germany, and international colleagues report the results in an early online edition and in the February issue of The Lancet Neurology.
DIAS-II was designed to confirm the previous results and further assess the safety and efficacy of desmoteplase. Patients who had acute ischemic stroke were included if they were randomized within three hours of symptom onset and had tissue at risk as defined by perfusion CT or diffusion/perfusion MRI. The efficacy of the treatments was assessed at 90 days with a composite clinical response score comprising three clinical indices of function and the amount of disability.
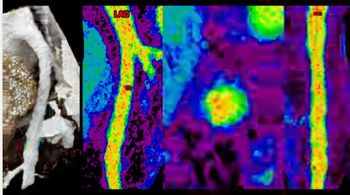
Patients were selected with the help of MR imaging techniques (perfusion imaging, diffusion-weighted imaging, or perfusion CT) that are thought to be able to distinguish the areas to which the supply of blood has been completely cut off (which are dead and unsalvageable) from the areas where the blood supply has been greatly reduced but the tissue could potentially be saved by timely restoration of the full blood supply (reperfusion). Patients who were deemed to have a high proportion of salvageable tissue relative to dead tissue (mismatch) were included.
The clinical response rates were low and there was no significant difference in outcome among the patients who received either dose of desmoteplase or placebo (47% for low-dose desmoteplase, 36% for high-dose desmoteplase, or 46% for placebo). The mortality rates were higher among patients who were given desmoteplase than in those given placebo (11% for low-dose desmoteplase, 21% for high-dose desmoteplase, and 6% for placebo), although the number of patients who had symptomatic intracranial hemorrhages was similar to that reported in the previous studies (4% in the low-dose group, 5% in the high-dose group, and no patients in the placebo group had this adverse effect).
The authors attributed the failure to replicate the results of the preceding studies mostly to the mild strokes recorded in the DIAS-2 group. "Small core lesions and small mismatch values that were associated with no vessel occlusion…could possibly reduce the potential to detect any effect of desmoteplase," they wrote.
In an accompanying comment, Dr. Michael Hill of the Calgary Stroke Program speculated that the DIAS trial may have forged too far ahead of the imaging science in its use of functional CT and MRI to select patients for treatment beyond the normal three-hour window. He expressed optimism that despite the results of DIAS-2, desmoteplase may yet prove to be the thrombolytic of choice if the lessons learned are applied to the DIAS-3 study.
For more information from the Diagnostic Imaging and SearchMedica archives:
Advertisement
Related Content
Advertisement











Advertisement
Advertisement
Trending on Diagnostic Imaging
1
Six Key Considerations on Aortic Dissection for Radiologists
2
SCCT: Should Photon-Counting CT Be the New Standard for Assessing CAD Prior to TAVR?
3
Competitive Eating: A New Niche for Radiologists?
4
SCCT: Pre-Pregnancy CAC Associated with Threefold Higher Risk of Preeclampsia
5