
|Slideshows|January 27, 2015
Elbow Swelling After Trauma
Author(s)Harpreet Singh, MD
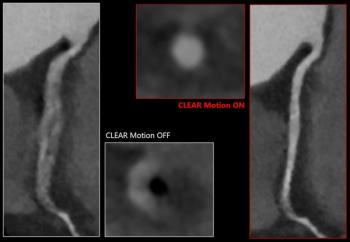
Case History: 22-year-old patient presented with complaint of swelling of elbow for six months following trauma.
Advertisement
Case History: 22-year-old patient presented with complaint of swelling of elbow for six months following trauma. MRI of elbow was performed.
Advertisement
Related Content
Advertisement












Advertisement
Advertisement
Trending on Diagnostic Imaging
1
Emerging PET/CT Radiopharmaceutical May Double Detection of Liver Foci in Patients with Neuroendocrine Tumors
2
AI in Radiology: Emerging Trends, Current Obstacles and Future Directions
3
Can the New PACS Viewer Bolster Efficiency in Radiology Workflows?
4
MRI and CT Data Show Improved Progression-Free Survival with Emerging Agent for Gastroenteropancreatic Neuroendocrine Tumors
5