

|Slideshows|February 23, 2016
Everything is Backwards
Author(s)Josh Gottlieb, OMSIII, Roy Gottlieb, DO, FSCCT
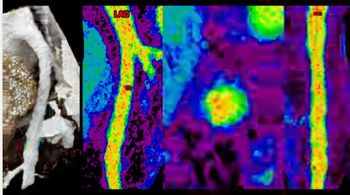
Case History: 68-year-old female with progressive shortness of breath, history of a complex congenital heart disorder.
Advertisement
Case History: A 68-year-old female with progressive shortness of breath and history of a complex congenital heart disorder has been followed over a cnumber of years.
Advertisement
Related Content
Advertisement











Advertisement
Advertisement
Trending on Diagnostic Imaging
1
Six Key Considerations on Aortic Dissection for Radiologists
2
Competitive Eating: A New Niche for Radiologists?
3
SCCT: Should Photon-Counting CT Be the New Standard for Assessing CAD Prior to TAVR?
4
SCCT: Pre-Pregnancy CAC Associated with Threefold Higher Risk of Preeclampsia
5