
|Articles|May 1, 2007
Healthcare IT spending jumps as China's growth accelerates
China's fast-growing economy is proving to be good news for the healthcare IT industry. Hospitals seeking to upgrade their standards of patient care and improve workflow are increasingly turning to digital solutions.
Advertisement
China's fast-growing economy is proving to be good news for the healthcare IT industry. Hospitals seeking to upgrade their standards of patient care and improve workflow are increasingly turning to digital solutions. The thirst for healthcare efficiency is such that total healthcare IT spending is expected to top 10 billion yuan (US$1.3 billion) by 2009, according to Clarence Wu, vice president and general manager for GE Healthcare IT solutions Asia.
"If you look at healthcare IT investment in China, it is actually growing faster than gross domestic product," he told delegates at the 2006 Asian Oceanian Congress of Radiology in Hong Kong.
One of the largest growth areas is digital image management. PACS was introduced in China approximately 10 years ago. Fast forward a decade, and the market for PACS and radiology information systems is growing at 30% per annum.
Wu credits a number of factors for driving the widespread adoption of PACS. The Chinese government is keen to see a high level of healthcare digitization by 2010. Large hospitals, which may handle up to 3000 outpatient appointments each day, strive to manage their workload more effectively. Abandoning film and processing chemicals should save money and have a positive environmental impact. PACS is regarded as an important tool in the battle against infectious diseases such as severe acute respiratory syndrome (SARS) and avian flu, as a result of its promise to speed up imaging-led diagnoses.
The nature of the specific PACS being purchased not surprisingly depends on the nature of the purchasing institution. China's level three university-affiliated facilities with at least 500 beds generally seek whole-hospital solutions, Wu said. These institutions want diagnostic-quality monitors in all departments where imaging is performed and, often, web-based image access in clinical departments and on the wards. Radiologists working in level three hospitals may also expect to find advanced applications such as 3D visualization tools in the PACS, as well as full integration with a RIS.
General community hospitals with 200 to 500 beds (level two) tend to offer PACS access within the radiology department alone. But these institutions are just as likely as the larger hospitals to seek a PACS/RIS.
"With the integrated PACS/RIS, they can get workflow benefits and make diagnoses more quickly. So they are still getting a significant benefit, although the PACS is only a departmental solution," Wu said.
Interest is also growing in linking multiple institutions together with a single imaging infrastructure. One such project, aimed at connecting 23 major hospitals in Shanghai, is currently out for tender. Storage will clearly be an important issue, though this will not be as challenging as might be expected, given the relatively low volume of imaging data generated by hospitals in China. The largest hospital in Guangdong province, with almost 2000 beds, for example, performs just 400,000 imaging procedures per year. A 1000 to 2000-bed site in the U.S. would probably perform over one million such examinations in the same period.
"Over time, we do foresee an increase in procedure volume within the hospitals, but computers are getting better and networks are improving, so there shouldn't be any major technical obstacles to doing this type of project in China," he said.
CLINICAL INTEGRATION
Another area where healthcare IT investment is soaring is the digitization of patient records. The market for electronic health records is less mature than that of PACS, and the installed base is smaller. The EHR has risen to prominence over the past two to three years, however, resulting in approximately 20% market growth.
The EHR and PACS markets are now quite separate. Purchasing decisions are generally made in different hospital departments, and integration between the systems is minimal. Most EHR systems in operation can document and handle patient test results and billing, but there is little advanced clinical functionality.
This scenario is likely to change in the future, as greater emphasis is placed on whole-hospital integration. Wu predicts that purchasers will seek single solutions combining the administrative and finance functions of a hospital information system and the management of all clinically relevant information in an EHR.
Tighter integration between the EHR and PACS will doubtless be part of this trend.
"You won't have to wait 10 years. I think that two or three years down the road, we are going to see a lot of this going on," Wu said.
IN-HOUSE OR OUTSOURCED?
With more than 500 healthcare IT providers competing for business in China, the market is not only busy but also highly competitive. Wu estimates that approximately 80% of hospitals seeking an EHR turn to vendors, with the remaining 20% creating an in-house solution. Over 90% of institutions implementing a PACS will purchase a system rather than building their own.
"Hospitals that build systems themselves, a lot of the time these are the bigger hospitals, so they can afford staff to build an IT solution for them. But we are seeing that they are running into issues with maintenance, support, and upgrades as the systems get older," he said.
Not all institutions are willing to abandon the homegrown approach just yet. For those preferring to retain control, a pick-and-mix route may be the answer, as the Hong Kong Hospital Authority has demonstrated.
Hong Kong's 43 public hospitals and 120 or so outpatient clinics are hooked up to an authority-wide clinical management system and electronic patient record (ePR) that was designed, built, and implemented entirely in-house. The ePR offers viewing access to radiological images acquired at 12 of the authority's 14 major hospitals, in part thanks to an archive server and DICOM viewer sourced from GE Healthcare.
Integration between individual hospitals' PACS and the ePR, however, and all project management have been handled by Hospital Authority IT personnel.
"Because the programming is done in-house, we have a lot of flexibility in how the system is developed to suit our own specific needs," said Dr. Ngai Tseung Cheung, executive manager of health informatics with the Hong Kong Hospital Authority. "Clinicians, radiologists, and administrators know that the system has been built around the way they work."
The project began in 1995 with the creation of clinical management system modules allowing clinicians to keep tabs on patient appointments and results, order tests and medication, and enter discharge summaries and reports. These different systems were merged into a unified ePR in 2000, so that doctors could call up all information on a particular patient, no matter where examinations or tests had been carried out.
Adding access to images was the next logical step, given that many radiology departments were going digital, Cheung said. Any doctor wishing to access the results of a radiological study can now simply click on a link in the ePR's radiology section. A selection of "reference quality" images stored in the central archive is then retrieved and displayed via the DICOM viewer. Radiologists seeking diagnostic-quality images still have access to uncompressed data stored in the local PACS archive.
Cooperation from clinicians and radiology staff has been vital to the system's success. Informatics staff first asked 160 clinicians to view a series of compressed images from different modalities and compare them with uncompressed versions of the same image. This provided a good indication of how much compression would be acceptable for reference quality. Relatively simple solutions were sought for the selection of key images to be sent to the central archive.
"For a CT scan, for example, if you are taking 1-mm slices, you will have hundreds of images. We don't send all of these to the centralized archive, but they will all be stored in the departmental PACS archive for volume reconstruction," Cheung said.
Incorporating access to compressed images within the ePR offered many advantages over a regional PACS project. Storage costs are lower because the central archive contains selected compressed images. A costly network upgrade was avoided, as was outlay on additional diagnostic-quality monitors. Additional cost savings are expected once radiology departments go completely filmless, a process about to be tested in a few of Hong Kong's public hospitals.
"What we are finding from our calculations is that you should be able to save enough money from not printing films to pay for the system itself. With a traditional PACS, I don't believe that is possible. You cannot save enough. You have to make a case based on intangible benefits," Cheung said.
Given the vast amount of image data accumulated in each PACS, these systems can be used to investigate innovative clinical service and research and education by applying the concept of imaging informatics, according to Dr. Bernie H.K. Huang of the Shanghai Institute of Technical Physics and the Image Processing and Informatics Laboratory at the University of South California.
"Medical imaging informatics is a relatively new academic discipline," he told AOCR attendees. "It utilizes basic knowledge in several established fields in engineering, computer science, physics, and related medical specialties. Its training requires a different type of approach compared to traditional disciplines."
He urged PACS users to consider investigating the Biomedical Imaging Informatics Training Program, which is supported by the National Institutes of Health. He also suggested that they make appropriate use of a DICOM-based image data grid, which is a service in the grid computing technology that can be used for medical image storage applications. It has applications in image-based clinical trials, combining teleradiology and PACS operations at the enterprise level, and fault-tolerant backup archive and disaster recovery of medical images.
PACS-based computer-aided diagnosis is also becoming a realistic option. CAD software can be used in a stand-alone workstation or be integrated in the PACS. Using the right software toolkit for the integration of CAD can address PACS workflow issues, as can using DICOM technology and Integrating the Healthcare Enterprise workflow profiles, Huang said.
Ms. Gould is a contributing editor of Diagnostic Imaging.
Advertisement
Related Content
Advertisement













Advertisement
Advertisement
Trending on Diagnostic Imaging
1
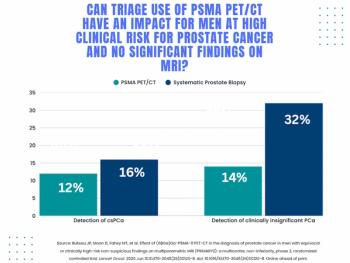
Study: PSMA PET/CT Reduces Biopsy Rate by Nearly 50 Percent for Men with Equivocal or Non-Suspicious Prostate mpMRI
2
Mammography Study: Can AI Detect Potential Breast Cancer Up to a Decade Prior to Diagnosis?
3
The Hidden Social Price of Remote Work in Radiology
4
Addressing Challenges in Radiology Reporting
5