

|Articles|July 1, 2009
Hepatobiliary, pancreatic MRimaging progresses at 3T
The spatial resolution of 1.5T MRI has beenimproved by parallel imaging and 3D gradient-echo sequences.
Advertisement
The spatial resolution of 1.5T MRI has been improved by parallel imaging and 3D gradient- echo sequences. Thin-slice images can also be obtained using 3D gradient-echo imaging. Both of these advances are relevant to dynamic imaging investigations of hepatobiliary and pancreatic disease using gadoliniumbased contrast media.
Three-D gradient-echo sequences include LAVA (liver acquisition with volume acceleration, GE Healthcare), VIBE (volumetric interpolated breath - hold examination, Siemens Medical Solutions), and THRIVE (T1 high - resolution isotropic volume examination, Philips Medical Systems).
Three-T MRI has been used clinically in Japan since 2005, and its features have been studied widely. Moving to 3T doubles the signal-to-noise ratio compared with 1.5T MRI. This SNR gain can be kept or traded for speed, spatial resolution, or both.1 Thin-slice images obtained at 3T using 3D gradient-echo sequences are consequently superior to those obtained at 1.5T.
We now conduct all of our MRI investigations of hepatobiliary and pancreatic disease on a 3T system (Signa H Dx, GE). Our routine protocol be gins with T1-, T2-, and diffusion - weighted MRI. Dynamic imaging is then carried out with a fat- suppressed 3D T1-weighted gradient-echo sequence using parallel imaging (LAVA) with the following parameters:
• repetition time (TR): 3.4 to 3.5 msec
• effective echo time (TE): 1.4 to 1.6 msec
• flip angle: 12°
• bandwidth: 80 to 125 Hz/pixel
• field-of-view: 350 mm2
• matrix: 320 x 192
• slice thickness: 1.4 mm
• reconstruction: 0.7 mm
• partitions: 220 to 240
• parallel acquisition: 2 to 2.5
All studies are conducted during breath - holding.
Acquisition times range from 25 to 28 seconds, depending on the matrix and the number of partitions. These parameters are modified according to patient stature. Oxygen via a nasal cannula (1 to 2 L/min) is routinely offered to patients who might otherwise have difficulty with the breath-hold requirements. No bowel preparation is used. A commercially available wraparound body array coil, consisting of eight linear elements in a left-to-right direction for both the anterior and posterior components, is placed around the abdomen.
The gadolinium agent (Magnevist, Bayer) is administered at a dose of 0.1 mmol/kg body weight. It is injected intravenously at a flow rate of 2 mL/sec, followed by a 20- mL saline flush (0.9% NaCl) using an MR-compatible power injector (Sonic Shot 50, Nemoto Kyorindo). Arterial, portal, and equilibrium phases are initiated after the peak aortic enhancement time (delays of five, 30, and 100 seconds, respectively) using the test injection technique.2
This thin-slice imaging technique makes it possible to perform multiplanar reformation (MPR), curved planar reformation (CPR), and MR angiography. All of these reconstructions, in addition to the source images, are produced on a commercially available work station (Centricity AW Suite 2.0, GE). Some cases show more prominent artifacts than others, namely susceptibility and motion artifacts. Susceptibility artifacts refer to the signal loss that occurs in gradient-echo images around metallic implants or surgical clips. These are much more pronounced at 3T than at lower field strengths. Motion artifacts, which are associated with respiration, cardiac motion, and bowel peristalsis, also tend to be more prominent on 3T MR images.
One of the main limitations of 3T MRI is the increase in specific absorption rate, which is a measure of energy deposition. Doubling the static magnetic field from 1.5T to 3T causes the SAR to increase by a factor of four. It has been reported that a reduction in flip angle can help prevent breaching of SAR limits .3 We have consequently reduced the flip angle on all sequences , especially gradient - echo imaging at 3T. The use of LAVA at 3T also allows high- resolution images to be generated, with decreased SAR and high SN R. Furthermore, any potential drawbacks of the technique were alleviated upon inspection of the hepatobiliary and pancreatic region.
MRI VERSUS MSCT
Both MRI and CT have been used to examine hepatobiliary and pancreatic disease. It is well known that CT offers high spatial resolution, while MRI has excellent contrast resolution.
The popularity of CT for he patobiliary and pancreatic imaging has increased following the development of multislice systems. Benefits of MSCT include increased scanning speed, routine use of thin collimation, improved spatial resolution and z-axis resolution during single breath- hold imaging, and improved workstation technology. It has also become easier to acquire MPR, CPR, and CT angiography data from thin - slice axial images. Previous studies have re ported on the clinical utility of 3D reconstructed images for evaluating the pancreaticobiliary tract, vascular mapping, tumor detection, and staging.4-8
The main advantage of MRI is its contrast resolution, which is superior to that of MSCT. Gadolinium - enhanced dynamic MRI has a higher sensitivity for the detection of small hepatocellular carcinomas and hypervascular lesions than CT.9- 12 Improvements in gradient strength and parallel processing techniques that reduce motion artifacts will make MRI acquisition even more attractive.13
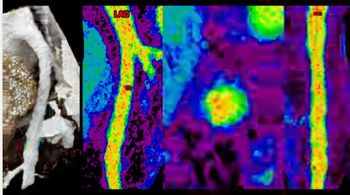
A high- resolution T1-weighted 3D gadolinium- enhanced MRI technique makes it possible to find small lesions and visualize their relationships with neighboring vessels and other structures. A longitudinal extension tumor such as cholangiocarcinoma, for example, can be identified on this type of reconstructed image.14 Some patients experience obstructive jaundice as a result of drainage tube insertion. MRI results in fewer artifacts from drainage tubes than MSCT (Figure 1).15
MRI allows simultaneous acquisition of results from common imaging techniques, such as T1-, T2-, and diffusion-weighted images and MR cholang iopancreatography. Patients are at risk of an allergic reaction or nephrotoxicity when iodinated CT contrast agents are used. Fewer complications have been reported during contrast - enhanced MRI examinations. Patients undergoing MRI also avoid exposure to ionizing radiation.
Thin - slice images from 3T MRI examinations may be more useful for diagnosis than those from multiphasic MSCT, provided that adequate image quality is maintained (Figures 2 and 3). The advantages of the LAVA sequence are high T1 contrast, thin contiguous sections with high SNR, and suppression of back ground tissues (Figures 2 and 3). On the other hand, we have found that, compared with MRA, CTA reveals more details of the small arteries, such as the peripheral than 1 mm can be obtained using MSCT, leading to significant improvements in terms of spatial resolution. MRI is equivalent, however, to MSCT in terms of portography and venography (
FUTURE APPLICATIONS
Arrays that are more sensitive and have multiring coils will be introduced in the future. These, together with flexible table movement at 3T, will permit imaging with an extended field - of- view and high spatial resolution. Future developments in 7T MRI will improve the quality of reconstructed images even more, allowing further detailed analysis of hepatobiliary and pancreatic disease.
Advertisement
Related Content
Advertisement











Advertisement
Advertisement
Trending on Diagnostic Imaging
1
Six Key Considerations on Aortic Dissection for Radiologists
2
Early Intervention for Coronary Artery Disease and the Role of Photon-Counting CT
3
SCCT: Should Photon-Counting CT Be the New Standard for Assessing CAD Prior to TAVR?
4
Interventional Radiology in Focus: A Closer Look at Y90 Radioembolization for Patients with Liver Cancer
5