
|Articles|July 24, 2012
Incomplete Documentation Shrinks Your Bottom Line
Author(s)Whitney L. Jackson
Poor documentation in your radiology reports may be to blame for your leaving rightfully-earned money unclaimed. Here’s where to look and how to boost revenue.
Advertisement
In the wake of the latest proposed radiology reimbursement cuts from CMS, documentation is more important than ever. And experts say your poor documentation may be to blame for your leaving rightfully-earned money unclaimed.
In fact, it’s common for radiologists to forego as much as 10 percent of overall legitimate revenue, according to Richard Duszak, MD, FACR, a radiologist with Mid-South Imaging and Therapeutics in Memphis and regular coding and billing columnist for the Journal of the American College of Radiology. While coders are your partners, they can only file for reimbursement based on the information you provide. It’s your responsibility, he said, to be vigilant.
“Each report must answer three questions: why, what, and how,” he said. “Not the clinical questions, but why did you do the exam, what is the clinical history of the body part imaged, and how was it imaged. Did you use plain films, was contrast present, how many views?”
Problem Areas to Watch
Incomplete documentation in three areas account for approximately 75 percent of unclaimed reimbursement, Duszak said. By addressing documentation problems with clinical history, the use of contrast, and ultrasound, you will likely see your revenue grow.
First, work with your hospital partners to examine how information is documented in the emergency room. Often, referring physicians relay information verbally, and it isn’t recorded in the patient record. Without a properly recorded clinical history, coders must code for the lowest level of reimbursement, and radiologists won’t receive proper payment.
Second, pay close attention to documenting when you use intravenous contrast agents with a CT or MRI study. Failing to notate when you do use contrast reduces both technical and the professional reimbursement.
“Simply failing to mention the introduction of contrast in a CT scan will lead to a loss of legitimate revenue – often as much as 20 percent,” Duszak said. “That adds up over time. Radiologists, as a rule, do a lot of these, so it becomes very significant.”
Third, when performing a
There are other areas where you could potentially be losing money, said Stacie Buck, president and senior consultant at Rad Rx, a coding consulting company that specializes in diagnostic and interventional radiology services. Fortunately, she said, the fixes are easy.
Always document the number and types of views in the body of the report to avoid having a claim down-coded. And, when documenting 3D reformatted images, note the medical necessity for obtaining them as 3D reformatting isn’t standard for MRI or CT exams.
The Coder’s Perspective
In most cases, Buck said, coders know radiologists are performing services that don’t appear in the documentation, but without written evidence, they can’t help you claim the revenue. “It is very frustrating to coders when they receive conflicting documentation or incomplete documentation,” she said. “It forces coders to down-code encounters, which, of course, costs a practice or facility money.”
Although it can cause a delay in reimbursement, coders also have the option to come back to you for additional information, said Shirley Breslin, client education and coding training manager for AdvantEdge Healthcare Services, a leading radiology billing company. The length of the delay, however, is up to you.
“Delays in payment depend on how willing a physician is to help us. Having to go back to the radiologist can slow down payment anywhere from three days to a couple of weeks,” she said. “Some radiologists are very conscious of the fact that it’s important to get documentation done and done right. But it really comes down to how well the doctor receives hearing that additional information is necessary.”
Strategies to Improve Documentation and Increase Revenue
Breslin, Duszak, and Buck all agreed the first and most significant step to proper documentation is education for both you and your coders. Breslin said she makes routine visits to clients to reinforce the importance of properly documenting services rendered and encourages them to connect with professional organizations to keep abreast of any reimbursement changes made to common procedures.
Duszak also recommended using templates to take the guess work out of dictation. Even if you get distracted while documenting your work, the template will prompt you to answer questions that are necessary for you to receive the correct reimbursement.
If you’re a group leader, your attitude toward proper documentation can often be the largest motivating factor for your colleagues, said Frank Smith, AHS’s vice president for client management.
“The head of a group can make a big difference,” he said. “If he or she treats documentation as important, then other doctors will pay attention, as well. If they don’t pay attention to it, we don’t get a very enthusiastic response for making any changes.”
Upcoming Changes Affecting Documentation
There are three looming changes that will make it even more important for you to document the services you provide correctly, said Bill Gilbert, AHS’s vice president for marketing at medical billing.
“Under the Affordable Care Act, in 2013 and 2014, more reimbursement will go to primary care. Specialties will receive less,” he said. “Radiologists have been at the forefront of reduced reimbursement for several years, and that will only continue or accelerate.”
The potential reduction in reimbursement to specialties stems from the CMS proposed Medicare Physician Fee Schedule for 2013 that calls for a 4 percent to 19 percent drop in radiology reimbursement rates. The move toward
In addition, Gilbert said, the advent of ICD-10, the next iteration of CMS coding effective in 2014, will require much more documentation in order to claim proper payment.
If you’re worried now, though, that you might be leaving money on the table when you file claims with CMS, Smith recommends you schedule an audit. It doesn’t have to be a huge, expensive undertaking - something small and relatively quick can suffice.
“You can do a fairly small audit on a small number of reports from five to 10 of your physicians,” he said. “It’s enough to get a very good idea of each individual’s documentation habits, as well as how the group does over all.”
One Hospital’s Experience
When Wisconsin’s Froedtert Hospital switched from film to digital imaging, the facility’s communication and documentation system crumbled, said Ann Gorman, the hospital’s radiology quality coordinator. The switch left the hospital without an effective way for the emergency department and trauma units to transfer information real-time to radiologists. Since then, updates to the PACS and RIS system have made proper documentation easier.
But without appropriate training, radiologists don’t know how to effectively use the documentation technology. To mitigate that problem, Froedtert’s leadership set aside four consecutive days of lunch time meetings in 2011 to address quality initiatives with providers. One session was devoted entirely to communication and the importance of complete documentation.
The result, said Charles Marn, MD, a Froedtert radiologist and Medical College of Wisconsin radiology professor, has been improved documentation and greater compliance among providers.
Proper documentation might begin with the individual radiologist, but the single practitioners aren’t solely responsible for ensuring all documentation is completed at a level that will maximize reimbursement.
“Radiologists can’t do all of this in a vacuum. Certainly, I’m the only one who can dictate my own reports, but there are people in the system who work with me as a team,” Duszak said. “Routinely documenting correctly will take looking beyond what the radiologist needs to do toward what the radiologist needs to do to be a successful part of a successful team.”
Advertisement
Related Content
Advertisement










Advertisement
Advertisement
Trending on Diagnostic Imaging
1
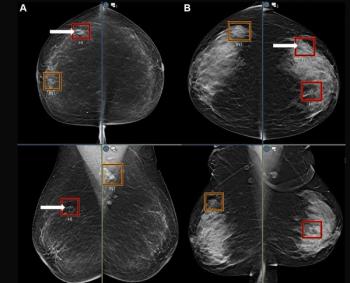
Mammography Study Suggests AI Can Bolster the Ability of General Radiologists to Detect Breast Cancer
2
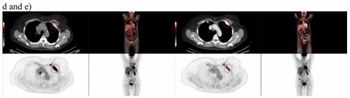
Study Suggests FDG-PET Better than CT for Assessing Treatment Response for Metastatic Breast Cancer
3
A Closer Look at the Evolution and Emerging Insights with Amyloid and Tau PET for Dementia and Alzheimer’s Disease
4
Could an Emerging Ultrasound Device Facilitate More Efficient Vascular Access Workflows?
5