|Articles|July 19, 2005
Long-term data validate thoracic aortic stenting
Endovascular repair could substitute for surgery as the standard of care for lesions of the descending thoracic aorta, according to a study presented at the 2005 Society of Interventional Radiology meeting.
Advertisement
Endovascular repair could substitute for surgery as the standard of care for lesions of the descending thoracic aorta, according to a study presented at the 2005 Society of Interventional Radiology meeting.
"EVAR provides a more effective single-step treatment than surgery," said principal investigator Dr. Fabrizio Fanelli, an interventional radiologist at the University of Rome La Sapienza.
Fanelli and colleagues reported on four-year data from 39 patients who underwent stenting for thoracic aortic disease. They found that EVAR was a better approach than surgery to treat type B thoracic aortic dissections and aneurysms.
Starting in November 2000, the investigators prospectively enrolled 28 patients with type B aortic dissection (15 acute, 13 chronic) and 11 patients with thoracic aneurysms. They achieved technical success in 26 of 28 dissections and immediate repair in all aneurysm cases.
At mean follow-up (25.8 months), no patients had experienced paraplegia, only two had suffered complications requiring surgery, and one had died of unrelated causes. All other patients remain alive and in good condition to date.
Despite EVAR's promising short- and midterm results, interventionalists have remained cautious. Fanelli's data, however, validate outcomes on stent-grafts' efficacy and safety two years or more after intervention.
Some issues remain. EVAR procedures are expensive, not all patients heal evenly, a significant percentage present with endoleak, and the long-term durability of stent-grafts has not been sufficiently established.
No consensus exists as to whether patients with aortic dissection should undergo treatment in the acute phase, after stabilization, or only when unstable. EVAR must be performed by expert teams of endovascular radiologists and cardiovascular surgeons in order to reduce complications deriving from technical mistakes, Fanelli said.
Despite the initial cost and potential complications, the shorter recovery period after EVAR brings down the overall costs associated with traditional surgery. The growing body of good results reported in the clinical literature may spur interventional radiologists to pursue this technique, according to Fanelli.
"Future application of this evolving technique may also allow the percutaneous treatment of type A dissections," he said.
For more information from the Diagnostic Imaging archives:
Advertisement
Related Content
Advertisement













Advertisement
Advertisement
Trending on Diagnostic Imaging
1
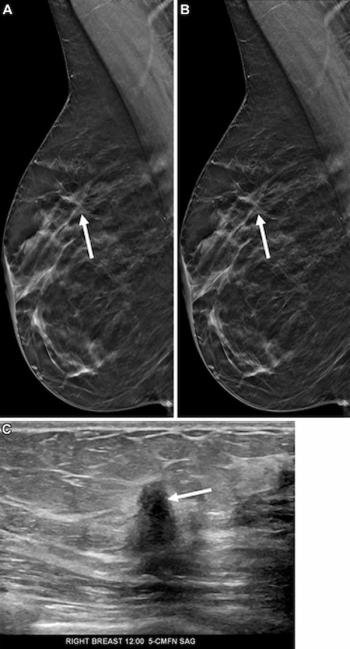
Mammography Study Shows Impact of AI-Powered Slab Reconstruction with DBT
2
SNMMI: What Early Research Reveals About the Alpha-Emitting Radioconjugate ATNM-400 for Prostate Cancer
3
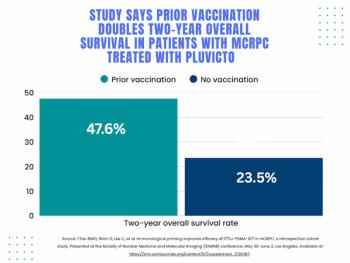
SNMMI: Does Vaccination Enhance Pluvicto Efficacy in mCRPC?
4
FDA Clears AI Ultrasound Software for Automated LVEF Calculation
5