|Articles|October 9, 2003
MGH pinpoints issues in PACS operations
The hot debate over the last decade was whether to acquire PACS. Now the question is simply how best to do it. Collective experience from early adopters is invaluable for optimizing PACS performance.One of the most important lessons of the last decade
Advertisement
The hot debate over the last decade was whether to acquire PACS. Now the question is simply how best to do it. Collective experience from early adopters is invaluable for optimizing PACS performance.
One of the most important lessons of the last decade is that the original conceptualization of PACS was far too limited. Visionaries of 20 and 30 years ago imagined the all-digital radiology department but did not envision the all-digital medical enterprise, with ubiquitous hospital networks and electronic medical records. Consequently, many early commercial PACS were designed as closed systems for the all-digital radiology department. Departments with these PACS have struggled to achieve fluid, rapid, and user-friendly enterprise image distribution. PACS design now centers on Web technology, which greatly facilitates the enterprise distribution requirement.
Resolution of the issue of enterprise image distribution is vital, and it must be accomplished before significant cost savings from reduction in film utilization can be realized. The goal in enterprise image distribution is a system that is integrated into the institution's electronic medical record, so that it is transparent to the clinician user at the point where images and reports are actually archived. Commercial PACS companies have been slow to recognize the importance of this level of integration, viewing their own respective systems as stand-alone.
The advent of PACS has also highlighted the central role and importance of the radiology information system. It is now clear that a sound, well-functioning RIS is a prerequisite to successful installation of PACS. Ideally, the RIS should be robustly integrated with the HIS, so that the hospital or enterprise master patient index (MPI) or central patient registration system can serve as the single "source of truth" for all patient demographic information. Institutions that have installed PACS without a RIS and/or without using a single MPI invariably struggle with misidentified patient records. This greatly reduces the functional value of the PACS and increases the risk of lost data. Medical legal exposure ensues. Experience has shown that it is better to take care of RIS issues and RIS/HIS integration first, even bearing the cost and time of replacing an outdated RIS if necessary, before embarking on PACS. As illustrated in the figure on page 31, the RIS is the "quarterback" for information management in radiology departments. A good PACS in no way substitutes or makes up for a bad RIS.
The historic inability to transfer patient and study information directly from the RIS to the respective imaging modalities is another major integration issue. The lack of a direct electronic connection from the RIS to a CT scanner or other imaging device requires technologists to reenter patient names and registration numbers at the console. This not only takes time and effort but is fraught with error. Mistakes in patient identification at the imaging device persist in the PACS, resulting in cases that cannot be resolved between the PACS and RIS. These cases stay in limbo until a PACS technologist can track down the mistake so the patient is correctly identified in the system. If cases are allowed to go into the PACS with identification errors, the patient records may be unretrievable. This comes as a shock to new PACS users. How can cases be "lost" in a computer!
Most digital imaging devices now being produced allow for the direct transmission of patient and study information from the RIS to the modality, resulting in error-free identification of the patient throughout the imaging process. Hospitals and radiology departments should recognize that optimum PACS performance will not be achieved until all imaging devices are converted to systems that allow electronic connectivity with the RIS, and through the RIS to the MPI.
We have coined the term "electronic round-trip" to describe the ideal goal of total connectivity from electronic order entry to electronic delivery of reports and images to referring physicians. Such electronic connectivity eliminates errors and reduces work effort. All patient identification data come from the MPI and are never reentered by hand at any step of the process. The goal is not just to install a PACS but to integrate it fully into the digital healthcare enterprise.
FINANCIAL INVESTMENT
One interesting debate over the last decade has been whether PACS pays for itself with a positive return on investment or costs money in perpetuity with a negative ROI. The good news is that more and more hospitals regard this question as moot. These institutions see PACS as the imaging component of the electronic medical record and recognize the positive functional impact. They see no reason to deny clinicians electronic access to image data when they are investing heavily in hospital information systems and electronic medical records. The bad news is that other institutions persist in looking at ROI.
The literature is split about whether PACS pays for itself, largely because methodologies, assumptions, and local conditions used in the analysis vary widely. The table on page 34 outlines a number of the factors that allow equally expert people to come to very different conclusions about PACS ROI. Hospitals that have already invested in physician workstations and associated networks suitable for PACS typically do not attribute these costs to PACS. Likewise, hospitals that have already recognized the quality and productivity benefits of computed radiography and direct capture digital radiography attribute these costs to the normal radiology capital replacement and upgrade process. Hospitals with suitable networks and clinician workstations in place are likely to greatly reduce the amount of film production and realize major savings from the cost of film, film processing, and film handling. Departments with high volumes of CT and MRI show the greatest benefit from reduced filming, while hospitals dominated by plain radiography benefit the least. The threshold costs for installing PACS favor a positive financial return for larger versus small institutions. Hospitals that implement voice recognition at the same time as PACS realize additional cost savings from eliminating the transcription process.
As indicated in the table, there are opposite ways to keep score for each of the parameters. Some institutions lack the cultural will to reduce the use of hard-copy film, or they may not have the network and desktop computer availability needed to deliver images to clinicians electronically, and this keeps them from realizing savings. By looking at these issues one by one and then carefully assessing how a particular ROI calculation has been made, it is easy to understand how conclusions differ. In the end, like many other financial analyses, there is no absolute right and wrong absent the assumptions that one institution decides to make versus another. Clearly, if all of the issues are tipped in favor of a positive ROI, PACS is a big winner. Likewise, if they are tipped to the negative, PACS will be a perpetual loser financially.
In particular, assumptions about the number and kinds of workstations required are major drivers of cost differences between PACS installations. We had a relatively modest budget to install PACS at MGH for a department performing more than 500,000 examinations per year. We were forced to find alternative solutions to simply adding more $40,000 reading devices at each state of implementation and found it essential to separate the display software application from the commodity display hardware to achieve serious savings in this area. Once separated, the software and hardware can be purchased and negotiated individually. While it is unlikely that a display application vendor other than the institution's PACS vendor would be chosen, software-only display applications can often be purchased through more affordable licensing methods from the same PACS vendor (e.g., software-only site licensing, browser access licensing, concurrent user licensing). Display hardware can be purchased from myriad manufacturers at a wide variety of costs and performance specifications and selected for its intended purpose: primary interpretation, clinical review, operating room viewing, office review, resident review, or technologist review. Typically, cost savings are tremendous.
WORKFLOW AND ARCHIVES
Workflow is a central PACS issue that was poorly understood 10 years ago and is still very much a work-in-progress. In a smaller work environment, or in a general radiology practice where everyone reads everything, workflow may not be such an issue. As departments get larger and the degree of subspecialization becomes more defined, workflow issues become magnified. The basic problem is to match each case coming through the PACS with the work list of a radiologist capable and responsible for interpreting that particular case or category of case.
One practical example that comes up routinely involves grouped or associated procedures such as a chest CT, abdominal CT, and pelvic CT-all obtained at one time from a single patient. In many subspecialized departments, the chest CT would be read by one radiologist and the abdominal and pelvic CTs by another. The PACS must have the intelligence built into it to allow these procedures to show up on two different work lists. Optimization of PACS requires transparent access to cases by the right radiologist, with all cases accounted for. The ease of accomplishing this, which varies greatly between systems, is worth considering.
Lower cost archives with improved performance are helping address workflow issues. It is now feasible to have far more of the total database immediately available online than it was five or 10 years ago. In the past, a PACS technician would have to pull prior images off a long-term archive to make them available for comparison with a current case. Now, however, old cases are available with the same speed and convenience as more recent ones, making the process completely transparent to the end user where the images are being stored. A 15-month archive available immediately online has turned out to be the practical minimum for optimum workflow. This minimum encompasses most episodes of acute illness and anything done at one-year follow-up. Obviously, more is always better.
One implication of faster archive response coupled with faster networks is the ability to access images on demand instead of requiring them to be pushed to a local cache first to allow rapid viewing. In a large department, the need to push images to workstations creates nothing short of a nightmare. To which and how many workstations should a study be sent? How do you guarantee availability of prior exams? How do you prioritize urgent cases? How do you know where each radiologist will be? Even though challenging aspects to sorting out workflow strategies remain, fast system response is the key. It allows cases to be "pulled" instead of "pushed," which reduces network traffic and permits great flexibility in parceling out cases to radiologists.
WORKSTATION FUNCTIONS
Parallel developments in image manipulation, including 3D renderings and computer-aided diagnostic applications, highlight another fundamental watershed in PACS development. Until now, all special image processing has typically required separate dedicated workstations, since most PACS companies have not provided image processing tools on their workstations beyond simple windowing, leveling, measurement and magnification tools, and some rudimentary 3D visualization techniques such as maximum intensity projection and multiplanar reformatting, thereby limiting what radiologists can do online. Sophisticated 3D and CAD analysis is now mostly done offline with specific 3D application software. This creates logistical problems in matching up the processed images with the original data sets. Many institutions, including MGH, simply append the processed images to the respective PACS files. This is clumsy and typically does not permit dynamic viewing of 3D renderings.
The open question now is whether advanced image processing will be incorporated in the PACS workstation with full utility available to the end user, either clinician or radiologist. For the full potential of image postprocessing to be realized, far more functionality must become available on the PACS workstation. PACS vendors-by their incorporation of exogenous 3D applications into their own PACS application software-are making increased functionality more available.
POOR COUSINS
Education, training, and system support are probably the poor relations in the entire PACS story to date. It is amazing that hospitals will invest hundreds of thousands and even millions of dollars in systems and routinely underestimate the training needs of support staff. An important lesson of the last 10 years is that PACS is not a turnkey system. It requires constant maintenance and vigilance to keep up and running. Servers crash, networks go down, workstations fail. Radiology departments will be well served to negotiate the right level of support internally from the hospital information services department and externally from the PACS vendor. Radiologists become frustrated and lose trust in technology that breaks down, especially if there is no prompt resolution.
Training is especially important for voice recognition. Of all the technologies that have come into radiology departments, this is the most difficult to learn. Radiologists who spend the time to truly train the system to their voices, learn how to use templates and macros, and master all of the system enhancements and shortcuts like voice recognition and would not go back to conventional transcription. Radiologists who fail to fully engage and never completely grasp the benefits of templates and macros will struggle with it and feel that it slows them down.
As more radiologists change their work from film to workstation image viewing, issues of work environment and ergonomics have also arisen. The ideal configuration for keyboard, mouse, voice recognition system microphone, diagnostic workstation monitors, and RIS/voice recognition monitor is still definitely a work-in-progress. Poor ergonomics can lead to fatigue and promote repetitive stress injury. Backlighting reduces effective image contrast, and excessive ambient noise can interfere with voice recognition. In general, PACS environments must be darker and quieter than film-based viewing environments. Simply converting an old room is often not the best solution.
The least well appreciated major quality assurance issue in PACS is monitor performance. The American College of Radiology has standards for monitor performance and a suggested approach to testing monitors. This approach should be incorporated into the routine maintenance program for any PACS, but it may often be overlooked. As the field migrates from CRTs to flat-panel displays and from medical-based to general-purpose devices, new methods and management strategies for QA and QC of display devices will be needed.
The benefits of PACS and voice recognition are obvious and considerable. The full realization of these benefits requires a systematic understanding of PACS components and their interrelationships and, beyond that, the integration of PACS into the digital healthcare enterprise.
Dr. Thrall is radiologist-in-chief, and Dr. Dreyer is vice chair of radiology, both at Massachusetts General Hospital.
Advertisement
Related Content
Advertisement












Advertisement
Advertisement
Trending on Diagnostic Imaging
1
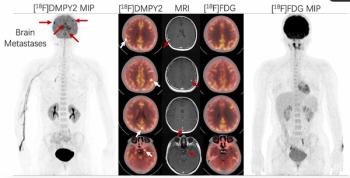
Molecular Imaging in Focus: Key Takeaways from the 2026 SNMMI Conference with Michael Hofman, MBBS, FRACP
2
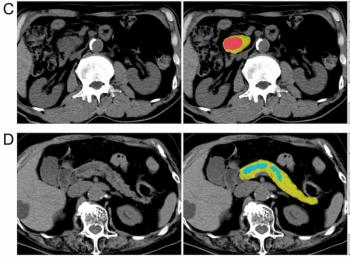
Can AI Enhance Non-Contrast and Contrast-Enhanced CT Detection of Pancreatic Cancer?
3
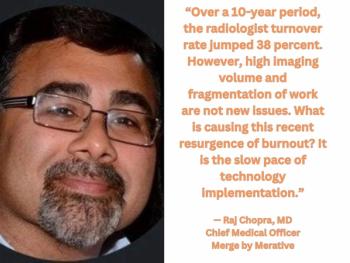
Five Strategies to Facilitate Technology Implementation and Alleviate Radiologist Turnover
4
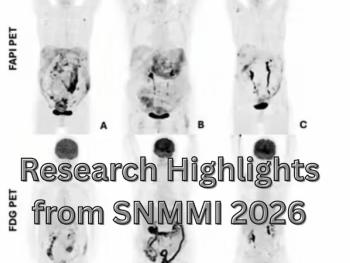
Research Highlights from SNMMI 2026
5