

|Articles|October 13, 2004
MSCT provides first- line colon assessment
Colorectal carcinoma is believed to be the third most common malignancy and the third leading cause of cancer-related deaths for men and women in Western countries. It is curable if detected at an early stage and preventable if precursor adenomatous polyps are detected and removed promptly.
Advertisement
Colorectal carcinoma is believed to be the third most common malignancy and the third leading cause of cancer-related deaths for men and women in Western countries.1 It is curable if detected at an early stage and preventable if precursor adenomatous polyps are detected and removed promptly.2
Diagnosis is traditionally based on conventional colonoscopy and/or double-contrast barium enema. Neither technique can assess the depth of bowel wall invasion, however, and both methods are severely limited in identifying lesions synchronous to the primary tumor.3
Several studies in the past decade that investigated the potential roles of CT and MR in the assessment of patients with colorectal carcinoma produced conflicting results.4-7 But these reports were limited by the use of past-generation scanners (nonspiral CT technology) and inadequate patient preparation (the colon was neither cleansed nor distended prior to examination).
The ideal colorectal cancer diagnostic test should have high sensitivity, high specificity, local staging capabilities (evaluation of the depth of invasion of primary neoplastic mass), distant staging capabilities (assessment of lymphadenopathies and/or metastases), and full colonic evaluation even for obstructive lesions. No preoperative examination meets all of these criteria.
Increasing interest has therefore focused on CT colonography (also known as virtual colonoscopy) as a potential tool for diagnosis and staging of colorectal carcinoma. This technique is based on the acquisition of spiral CT data sets of an air-distended cleansed colon. The data are subsequently postprocessed on dedicated workstations to generate 2D and 3D endoscopic-like images of the colon.8-10
Numerous studies of CT colonography have demonstrated excellent results in lesion detection,8-10 surgical follow-up,11 and patient acceptance.12 One study has also shown CT colonography to be suitable as a screening tool for colorectal neoplasia.13
OPTIMUM TECHNIQUE
CT colonography is similar to a standard abdominal/pelvic CT scan, although several important factors differentiate the two examinations. Patients undergoing CT colonography must ingest a cathartic preparation such as polyethylene glycol, Fosfosoda, or magnesium citrate the day before the examination. These preparations are also used for standard colonoscopy and double-contrast barium enema examinations. Inadequate bowel cleansing can lead to false-negative results on CT colonography if lesions are obscured by fecal matter or false-positive results if waste products simulate lesions.
10
This onerous bowel preparation restricts the use of CT colonography considerably, and several strategies have been proposed to avoid this step.14,15 CT colonography is unlikely to demonstrate sufficiently high patient compliance for use in screening unless the need for cathartic preparation is eliminated.
The colon has to be distended prior to CT colonography to prevent collapsed bowel segments from obscuring underlying disease. Distention is often achieved by insertion of a small rubber catheter into the rectum, through which air or carbon dioxide is administered. Insufflation must be performed carefully by a nurse or radiologist until maximum patient tolerance is reached. Colonic distention is reportedly one of the worst parts of the examination for patients,12 but no major complications related to insufflation have been reported in the literature.
A further distinctive feature of CT colonography is intravenous administration of antiperistaltic drugs, either hyoscine butylbromide or glucagon hydrochloride, prior to examination. The use of an antiperistaltic agent minimizes bowel spasm, thus reducing the incidence of bowel collapse and increasing the quality of CT colonography results. The drugs should also theoretically reduce discomfort associated with colonic distention.
Radiologists have yet to reach agreement on the routine use of antiperistaltic drugs with CT colonography. We have found that neither hyoscine butylbromide nor glucagon hydrochloride improves colonic distension, though administration of either reduces patient discomfort substantially.16 We now use hyoscine butylbromide prior to CT colonography at our hospital, unless it is contraindicated.
CT colonography is performed in both the prone and supine positions, unlike standard abdominal and pelvic CT scans. Double acquisition is crucial to differentiating real lesions (polyps or carcinomas) from residual fecal material and thus to improving specificity.17 A lesion's position remains unchanged when the patient is turned, whereas fecal matter moves during repositioning. Moving a patient from the prone to the supine decubitus also allows redistribution of insufflated air within the colon, and poorly distended segments are often better visualized during the second acquisition.
Routine use of double acquisition has raised concerns about the ionizing radiation burden associated with CT colonography. This issue is of paramount importance if the test is proposed for screening. A number of radiation dose reduction strategies have already been investigated.18 All screening CT colonography examinations at our hospital are performed with an optimized low-dose technique that delivers a total radiation exposure of 1.8 mSv for men and 2.4 mSv for women. This is substantially lower than the radiation dose from a barium enema, which ranges from 3 to 7 mSv. Radiation concerns are clearly less important when a patient with known or strongly suspected colorectal carcinoma is referred for CT colonography. The purpose of CT colonography in such patients is to produce images of the highest diagnostic quality to assess precisely the presence of local and distant disease.
We use a high-resolution protocol when performing nonscreening CT colonography on a Siemens Somatom Plus 4 Volume Zoom machine (1-mm slice collimation, 1-mm slice thickness, 1-mm reconstruction interval, 8-mm/sec table speed, 120 kVp, 80 mAs for prone acquisition, 165 mAs for supine). Contrast material is not used routinely in our hospital. For the purposes of local and distant tumor staging, however, IV contrast is administered to all patients referred for colorectal carcinoma and in all cases in which a mass is identified on transverse CT images obtained after the prone acquisition. IV administration during supine acquisition comprises 120 to 150 mL nonionic iodinated contrast, with an infusion rate of 3 mL/sec.
We transfer CT colonography data sets to a dedicated workstation for postprocessing. Image analysis is performed using a software package with volume rendering capabilities (Vitrea 2, Vital Images). Readers first analyze 2D axial images, moving to 2D multiplanar reconstructions and 3D images only when a suspected abnormality is detected. These additional views are used to confirm the suspicious finding and increase diagnostic confidence.
ADVANTAGES AND LIMITATIONS
MSCT has several advantages for colorectal carcinoma diagnosis and staging. The combination of prone and supine images provides a complete colonic evaluation in virtually all patients, even when an obstructive neoplasm is present.
19-21
CT colonography not only can detect the primary carcinoma, but it also depicts synchronous lesions, whether carcinomas or coexisting polyps (Figure 1). This feature is of paramount importance because the presence of a synchronous lesion can alter the surgical approach.
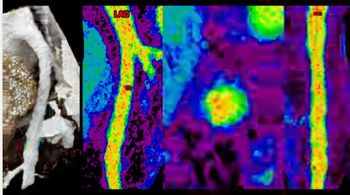
CT colonography offers a more precise description of lesion location than other diagnostic tests, especially conventional colonoscopy (Figure 2). Multiplanar reconstructions are especially helpful in depicting a tumor's location and extent of invasion. Contrast-enhanced CT colonography studies also permit assessment of tumor bowel wall invasion (local staging), and the presence of extracolonic disease such as lymphadenopathies and/or metastases (distant staging) (Figure 3). CT colonography provides a complete preoperative evaluation of patients affected by colorectal carcinoma.
But the technique still has several limitations. CT is not sufficiently sensitive to detect microscopic extramural tumor extension into fat surrounding the colon. This may lead to understaging, especially in the case of T3 tumors. A CT colonography scan is also incapable of distinguishing different layers of the bowel wall, making it extremely difficult to differentiate a T1 from a T2 tumor.
MSCT has further problems in differentiating stenosis due to diverticulitis from obstructive colorectal carcinoma. Imaging features used to differentiate these conditions include the presence of pericolic fat stranding to indicate inflammation or edema, and satellite lymphadenopathies that are highly consistent with malignancy.22 In many cases, however, radiologists find overlapping CT features; histological samples may then be required to reach definitive diagnosis.
Lymph node characterization is another limitation of CT colonography. Benign nodes may be enlarged, whereas subcentimeter nodes may contain metastatic tumor.
Despite these drawbacks, we consider MSCT colonography an excellent tool for detection and staging of colorectal carcinoma. Considering the current limitations of other available techniques, MSCT colonography can be proposed as a first-line diagnostic test for a complete evaluation of patients with colorectal carcinoma.
References
1. Jemal A, Murray T, Samuels A, et al. Cancer statistics, 2003. CA Cancer J Clin 2003;53(1):5-26.
2. Iyer RB, Silverman PM, DuBrow RA, Charnsangavej C. Imaging in the diagnosis, staging, and follow-up of colorectal cancer. AJR 2002;179(1):3-13.
3. Tate JJT, Rawlinson J, Royle GT, et al. Preoperative or postoperative colonic examination for synchronous lesions in colorectal cancer. Br J Surg 1988; 75:1016-1018
4. Freeny PC, Marks WM, Ryan JA. Colorectal carcinoma evaluation with CT: preoperative staging and detection of postoperative recurrence. Radiology 1986;158(2):347-353.
5. Zerhouni EA, Rutter C, Hamilton SR, et al. CT and MR imaging of colorectal carcinoma: report of the Radiology Diagnostic Oncology Group II. Radiology 1986;200(2):443-451.
6. Balthazar AJ, Megibow AJ, Hulnick D, Naidich DP. Carcinoma of the colon: detection and preoperative staging by CT. AJR 1988;150(2):301-306.
7. Hundt W, Braunschweig R, Reiser M. Evaluation of spiral CT in staging of colon rectum carcinoma. Europ Radiol 1999;9(1):74-84.
8. Fenlon HM, Nunes DP, Schroy PC III, et al. A comparison of virtual and conventional colonoscopy for the detection of colorectal polyps. NEJM 1999;341(29):1496-1503. Erratum in NEJM 2000;342(7)524.
9. Yee J, Akerkar GA, Hung RK, et al. Colorectal neoplasia: performance characteristics of CT colonography for detection in 300 patients: Radiology 2001;219(3):685-692.
10. Laghi A, Iannaccone R, Carbone I, et al. Detection of colorectal lesions with virtual computed tomographic colonography. Am J Surg 2002;183(2):124-131.
11. Laghi A, Iannaccone R, Bria E, et al. Contrast-enhanced computed tomographic colonography in the follow-up of colorectal cancer patients: a feasibility study. Europ Radiol 2003;13(4):883-889.
12. Svensson MH, Svensson E, Lasson A, Hellstrom M. Patient acceptance of CT colonography and conventional colonoscopy: prospective comparative study in patients with or suspected having colorectal disease. Radiology 2002;222(7):337-345.
13. Pickhardt PJ, Choi JR, Hwang I, et al. Computed tomographic virtual colonoscopy to screen for colorectal neoplasia in asymptomatic adults. NEJM 2003(23);349:2191-2200.
14. Callstrom MR, Johnson CD, Fletcher JG, et al. CT colonography without cathartic preparation: feasibility study. Radiology 2001;219(3):693-698.
15. Zalis ME, Perumpillichira J, Del Frate C, Hahn PF. CT colonography: digital subtraction bowel cleansing with mucosal reconstruction initial observations. Radiology 2003;226(3): 911-917.
16. Iannaccone R, Laghi A, Catalano C, et al. Role of glucagon and hyoscine butylbromide in CT colonography: a placebo-controlled study. Presented at annual meeting of RSNA, Chicago, IL; Dec 2003:212.
17. Yee J, Kumar NN, Hung RK, et al. Comparison of supine and prone scanning separately and in combination at CT colonography. Radiology 2003;226:653-661.
18. Iannaccone R, Laghi A, Catalano C, et al. Detection of colorectal lesions: lower-dose multi-detector row helical CT colonography compared with conventional colonoscopy. Radiology 2003;229(3):775-781.
19. Fenlon HM, McAneny DB, Nunes DP, et al. Occlusive colon carcinoma: virtual colonoscopy in the preoperative evaluation of the proximal colon. Radiology 1999;210(2):423-428.
20. Morrin MM, Farrell RJ, Raptopoulos V, et al. Role of virtual computed tomographic colonography in patients with colorectal cancers and obstructing colorectal lesions. Dis Colon Rectum 2000;43(3):303-311.
21. Neri E, Giusti P, Battolla L, et al. Colorectal cancer: role of CT colonography in preoperative evaluation after incomplete colonoscopy. Radiology 2002;223(3):615-619.
22. Chintapalli KN, Chopra S, Ghiatas AA, et al. Diverticulitis versus colon cancer: differentiation with helical CT findings. Radiology 1999;210(2):429-435.
DR. IANNACCONE and DR. LAGHI are radiologists, and PROF. PASSARIELLO is head of the department of radiological sciences, at University of Rome La Sapienza. Assisting in the preparation of this article were CARLO CATALANO, FILIPPO MANGIAPANE, and DANIELE MARIN.
Advertisement
Related Content
Advertisement











Advertisement
Advertisement
Trending on Diagnostic Imaging
1
FDA Clears AI-Enabled Ultrasound for High-Volume Clinical Settings
2
Diagnostic Imaging's Weekly Scan: July 5 — July 11
3
SCCT: Should Photon-Counting CT Be the New Standard for Assessing CAD Prior to TAVR?
4
Study Finds Nearly Fourfold Higher Neurodegenerative Mortality Rates for Former NFL Players
5