
|Articles|March 9, 2007
Multislice CT and microbubble sonography target inflammation in the small bowel
Recent innovations in multislice computed tomography (MSCT) and contrast-enhanced ultrasound have so dramatically improved the visualization of the small bowel wall and its vascularity that they are challenging the conventional workup of patients with acute or chronic inflammatory processes such as Crohn's disease.
Advertisement
Recent innovations in multislice computed tomography (MSCT) and contrast-enhanced ultrasound have so dramatically improved the visualization of the small bowel wall and its vascularity that they are challenging the conventional workup of patients with acute or chronic inflammatory processes such as Crohn's disease.
"Multiple studies have demonstrated that traditional fluoroscopic interrogation of the small bowel is lacking in its ability to detect pathology. So high spatial resolution CT techniques are emerging that can compete with and complement findings from capsule endoscopy," said Dr. Joel Fletcher, an associate professor of radiology at the Mayo Clinic in Rochester, MN.
One of these techniques, CT enterography, is highly sensitive and specific for Crohn's disease, and it is increasingly being used to stage the small bowel.
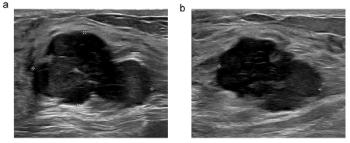
Contrast ultrasound versus enteroclysis. The enteroclysis clearly shows the stricture of the terminal loop of the small bowel without providing any information about bowel wall morphology and vascularity. Contrast-enhanced ultrasound shows the thickened bowel wall with increased vascularity after microbubble injection. (Provided by E. Quaia)
"A multiphase CT enterography examination with bolus tracking picks up many of the same patients as the capsule, and it picks up patients that the capsule thought were negative. So gastroenterologists are using it not as a replacement test but as a complementary one," Fletcher added.
Contrast-enhanced ultrasound is another method that can assess the status of small bowel wall vascularity due to its extremely high sensitivity to the microbubble harmonic signal of specialized contrast-specific techniques, noted Dr. Emilio Quaia from the department of radiology at the Cattinara Hospital, University of Trieste, in Italy. He was scheduled to discuss the procedure at this morning's special focus session on multimodality small bowel imaging.
Contrast ultrasound versus CT. The thickened terminal loop is clearly depicted by both contrast-enhanced ultrasound and CT enteroclysis, even though contrast-enhanced ultrasound provides superior depiction of the increased vascularity of the bowel wall. (Provided by E. Quaia)
CT enterography, which is a high spatial resolution CT of the abdomen and pelvis performed after a patient has ingested large amounts of enteric contrast, yields exquisite images of the small bowel lumen and wall, Fletcher said. Because of its robustness, it can be performed well in a variety of practice settings on a wide range of patients.
The technique must be optimized, however, in order to produce images of the highest quality. One factor involves delivery of the enteric contrast agent, which must be timed so the small bowel is distended at the time of scanning. Another is the choice of slice thickness and orientation to maximize z-axis spatial resolution. He recommends obtaining slices of 3 mm or less and reviewing multiplanar images rather than relying solely on axial scans.
Nevertheless, CT enterography should be used with caution in patients with Crohn's disease, because of the risk of repeated exposure to radiation. Fletcher gives three examples. If a patient has signs of a fistula or abscess, such as an elevated sedimentation rate and C-reactive protein level, the radiation dose of CT enterography is justified because of the possibility that the underlying pathology could spill bacteria into the blood and cause sepsis. If a young patient is being investigated to determine if he or she has Crohn's disease, then a one-time CT examination is warranted. However, if a clinician wants to see whether a newly prescribed medication is working, MRI is the better imaging choice, he said.
Sonography with sulphur hexafluoride-filled microbubbles allows real-time assessment of the bowel wall, produces spatial and contrast resolution that rival those of CT and MRI, and achieves the highest time resolution of all the imaging techniques, Quaia said.
Especially relevant for patients with Crohn's disease is the ability of contrast-enhanced ultrasound to provide functional information about bowel wall vascularity.
"In the active phase, the bowel wall presents diffuse vascularity, often involving the mesentery, or an increased vascularity at the level of the mucosa and submucosa. Contrast-enhanced ultrasound is very useful for a global assessment of the bowel wall vascularity, in particular at the level of the last bowel loop," Quaia said.
Contrast-enhanced ultrasound is not as effective as CT or MRI in identifying mucosal lesions or making a global evaluation of the small bowel, because sonograms are focused on a specific loop.
"However, contrast-enhanced ultrasound presents a superior sensitivity and temporal resolution in the assessment of bowel wall vascularity, which is the real strength of the technique," he said.
In the future, Quaia predicts, contrast-enhanced ultrasound will be used to evaluate the efficacy of medical treatment aimed at reducing bowel wall vascularity in patients with chronic inflammatory disease.
Lying ahead for CT enterography is the possibility of truly quantifying the active burden of Crohn's disease.
"With high spatial resolution data sets, we should be able to help clinicians determine the extent of the disease, measure the length of diseased segments, look for findings of Crohn's disease, and quantitate them. There is an endoscopic index of disease severity. We should be able to do the same thing with CT," Fletcher said.
Advertisement
Related Content
Advertisement










Advertisement
Advertisement
Trending on Diagnostic Imaging
1
Emerging PET/CT Radiopharmaceutical May Double Detection of Liver Foci in Patients with Neuroendocrine Tumors
2
What If a Radiologist Who Specializes in Blocking Unnecessary Imaging Requests Was Added to Your Practice?
3
Breast Cancer Screening: Where Things Stand
4
Can Contrast-Enhanced Mammography Improve Breast Cancer Staging?: Nine Takeaways from a New Literature Review
5