

|Articles|October 5, 2005
Perfusion-diffusion confusion yields to spatial information
In recent years, the use of MR perfusion- and diffusion-based imaging to predict tissue outcome following acute ischemic stroke has increased significantly. While most strategies to improve outcome have focused on MRI parameters, researchers from Boston and Finland have devised a novel approach that also includes spatial information.
Advertisement
In recent years, the use of MR perfusion- and diffusion-based imaging to predict tissue outcome following acute ischemic stroke has increased significantly. While most strategies to improve outcome have focused on MRI parameters, researchers from Boston and Finland have devised a novel approach that also includes spatial information.
The whole idea of the perfusion-diffusion mismatch has moved into the clinical mainstream. The approach is well replicated, and the mismatches can be correlated with likelihood of outcome, according to Dr. A. Gregory Sorensen, director of the Massachusetts General Hospital Center for Biomarkers in Imaging and coauthor of a study presented at the International Society for Magnetic Resonance in Medicine meeting in May.
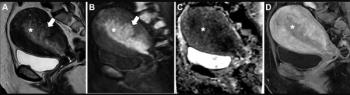
But this model produces six different images, including the apparent diffusion coefficient (ADC), cerebral blood volume (CBV), cerebral blood flow (CBF), and mean transit time (MTT), which makes fast interpretation difficult.
Spatial location is important in determining outcome, but modeling voxel location is a complex function. Researchers circumvented that problem by measuring the relative distance between the diffusion and perfusion abnormalities.
Nina M. Menezes, Ph.D., a radiology researcher at MGH, and colleagues from MGH and Kuopio University Hospital in Finland included in the study 75 patients who had undergone acute MR imaging within 12 hours following the onset of first-ever ischemic stroke and follow-up imaging a minimum of five days later. They created an "MRI-only" risk map constructed from six parameters, including the ADC and T2 maps from diffusion-weighted imaging; CBV, CBF, and MTT from perfusion imaging; and diffusion and perfusion images coregistered to each other and to patients' follow-up T2 images. They then created another risk map by adding a spatial component-the distance from the acute DWI lesion for each voxel-to the MRI-only parameters. Acute DWI were obtained using a b-value of 1000. From these, apparent diffusion coefficient and T2 (b = 0) maps were calculated.
The spatial model outperformed the MRI-only model in 68 patients. The MRI-only model resulted in an area under the curve of 0.75, whereas the inclusion of spatial information significantly increased the mean area under the curve to 0.83. With specificity fixed at 70%, sensitivity improved from 68% for the MRI-only model to 79% for the spatial model, a significant difference.
Advertisement
Related Content
Advertisement











Advertisement
Advertisement
Trending on Diagnostic Imaging
1
Emerging PET/CT Radiopharmaceutical May Double Detection of Liver Foci in Patients with Neuroendocrine Tumors
2
AI in Radiology: Emerging Trends, Current Obstacles and Future Directions
3
MRI and CT Data Show Improved Progression-Free Survival with Emerging Agent for Gastroenteropancreatic Neuroendocrine Tumors
4
Can the New PACS Viewer Bolster Efficiency in Radiology Workflows?
5