
|Articles|January 27, 2012
Q&A: Imaging Center Partners with Mobile Anesthesia Unit
Author(s)Diagnostic Imaging Staff
Diagnostic Imaging recently spoke with Dr. Rahul Desia, director of interventional pain management at EPIC Imaging, about their experiences with a mobile anesthesia unit.
Advertisement
As EPIC Imaging’s interventional pain management unit expanded, so did the need for anesthesia services. The imaging center, which has four locations in the Portland, Ore. area, provides imaging-guided diagnostic exams and therapeutic injections for relief of chronic pain and sports injuries.
When directors determined the on-staff registered nurse wasn’t enough, they opted for a mobile unit from Anesthesiology Associates Northwest, to provide on-demand staff and supplies. Diagnostic Imaging recently spoke with Dr. Rahul Desia, director of interventional pain management at EPIC Imaging, about their experiences with a mobile unit.
First can you detail what kind of anesthesia services you were providing before the mobile unit?
Yes, we did have a registered nurse that provided some oral and minimal IV sedation, but really we weren’t utilizing it that much before we were using the Anesthesiology Associates Northwest. I had just started maybe two months before having them on board. We just started the pain management division before that.
What made you decide to opt for a mobile anesthesia unit?
Simplicity, ease of use. You can call them and have them come out when you need to and not have someone on staff we might not be properly utilizing. They bill everything themselves. They take care of that, so it’s easy on my staff to focus on our own patients. We are an outpatient imaging center and we have a pain mgmt practice so we don’t have the accessibility like a hospital might have for anesthesia, so it bridges the gap we sometimes have.
So how does it work?
We usually know [when we will need anesthesia services], we are usually several weeks out for scheduling but at least a couple of days. We try to group cases that require sedation then I will have them available. We will try to stack two or three or four patients in a row where they can come in and take care of our patients.
What do the patients think?
It is transparent to them; they don’t know it’s a mobile unit. They know they are being taken care of an anesthesiologist or a [certified registered nurse anesthetist] and they are getting top quality care so they like it.
Do you have any advice for other imaging centers that are considering something like this?
It’s a great resource to have, it’s a minimal output, or minimal effort from our standpoint to have good quality care. We don’t have to use huge resources to hire a nurse or a [certified registered nurse anesthetist]. It also de-stresses our staff because they don’t have to worry about that aspect of it. We looked into several options. We do have a nurse on staff but we have 200 employees so [the nurse] is doing a lot of other things. And it’s a little outside their comfort zone.
Advertisement
Related Content
Advertisement













Advertisement
Advertisement
Trending on Diagnostic Imaging
1
Diagnostic Imaging’s Weekly Scan: June 14 — June 20
2
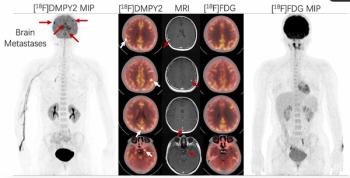
Emerging PET Radiotracer May Enhance Detection of Small Metastases in Patients with Advanced Melanoma
3
Molecular Imaging in Focus: Key Takeaways from the 2026 SNMMI Conference with Michael Hofman, MBBS, FRACP
4
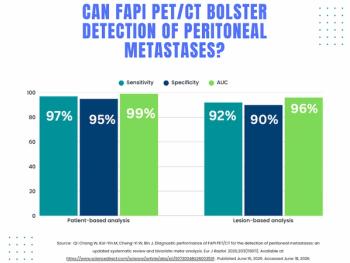
What a Meta-Analysis Reveals About FAPI PET/CT for Detection of Peritoneal Metastases
5