
|Articles|May 17, 2012
Q&A: Implementing Contrast-enhanced Spectral Mammography
Author(s)Sara Michael
Kristi Funk, MD, of the Pink Lotus Breast Center explains the benefits of CESM, the implementation of GE’s SenoBright technology, and the reaction from her patients.
Advertisement
The Pink Lotus Breast Center in Beverly Hills, Calif., recently became the first commercial institution in the U.S. to install GE Healthcare’s contrast-enhanced spectral mammography technology, SenoBright. GE’s system, which launched in 2010 and received FDA clearance in October 2011, produces contrast-enhanced images of the breast using an X-ray contrast agent and a dual energy acquisition technique.
Contrast-enhanced spectral mammography (CESM) creates two separate exposures per view of each breast, one showing tissue like the standard mammography and the other showing the iodine contrast to help the radiologist localize lesions. The procedure can be done on the same day using the same GE equipment, which cuts down on wait time for patients and lessens any burden on the practice’s work flow.
Diagnostic Imaging recently spoke with the Pink Lotus Breast Cancer's Kristi Funk, MD, about implementing the SenoBright system. Here’s the edited and condensed conversation.
What made you all decide to adopt this technology?
Until SenoBright came along, the Pink Lotus Breast Center was lacking one key component to our arsenal of diagnosis and screening and diagnosis and treatment of breast cancer, and that was a cost effective and yet sensitive and specific study for detecting cancer. We had mammography and ultrasound and our expert hands, and that was it. For us CESM completed the gap. It provided a way to resolve inconclusive mammography and ultrasound in a way that was still onsite and fully comprehensive under our own roof. The other big option until now had been MRI and for a variety of reasons we just felt from the perspective of longevity and sustainability, MRI was not the future and it wasn’t going to maintain itself, so we waited.
Tell me more about why MRI wasn’t the best path and how CESM compares to MRI.
[MRI] could never be reduced to a short enough time and remove all the labor intensive components to read MRI accurately. It requires a radiologist dedicated to reading just MR and preferably breast MR. The procedure itself takes an average of 45 minutes and with the IV start the person is there for a couple hours. You will never get to the level where we can screen the mass millions of women in the U.S. It’s not a general screening tool and I knew mammography had to go to the next level .
Right now the FDA has approved CESM for “an inconclusive mammogram and ultrasound,” so the next step prior to CESM would be an MRI. Given that CESM is just a quick IV injection of contrast and you get two views on each breast and that’s it. Ten minutes in and out with immediate answers and results.
It’s my hope and expectation that once this technology gains traction with more centers throughout the U.S. and more studies to show head-to-head comparison between routine digital as it is now and between CESM and MRI, it will be inconceivable not to implement this as screening for the masses.
I think some of the CESM will be reimbursed by some insurance companies. Part or all of the test would be reimbursed for people who have dense breasts, BRCA carriers, extremely strong family history, personal history of cancer - those are the people who are already at more than a 20 percent lifetime risk, therefore MRI is usually covered. I bet you it won’t be long before insurance covers that population and then the next step will be everybody.
Have there been any work flow changes at your center with CESM?
This is the beauty of incorporating CESM. All it is is a technology application that is uploaded into an existing mammo center. It fits beautifully in the work flow. We have allowed more time than a diagnostic mammo slot right now until we are really into the swing of things, but by and large it takes no more time than a diagnostic mammogram and you don’t need one new person with an extra skill. We didn’t hire anybody else.
What are your patients saying?
The ones who are the most relieved and grateful for this study are the ones with an abnormal MRI. We’ve been able to resolve some inconclusive findings that persist through MRI when you still have a normal ultrasound, and depending on which way the imaging flow went, your mammogram was either normal or abnormal, and them MRI didn’t help resolve that issue.
We’ve used CESM successfully on at least 20 occasions to create some peace of mind with a strong comfort level to either do a six-month follow-up or to corroborate with MRI to say, ‘You know what, there is something going on, let’s biopsy.’
We have found it’s really a beautiful adjunct to the existing modalities. I am not ready to throw MRI to the curb completely. There’s an important list of differences that add up to a more cost effective exam and a more comfortable exam.
And the biggest thing to me in terms of wanting to get my patients answers quickly is that MRI really needs to be timed to the menstrual cycle, and/or if you’re on hormone replacement you need to stop it for a minimum of three weeks. Otherwise you’re going to be fraught with false positives on the final MRI.
But [with CESM] the day you get an abnormal mammogram, you’re just coming in for your routine and we see it’s abnormal, we back up put the IV in do it again. And you leave with answers and a plan. There’s no two, three, six, eight weeks of deciding that you have to figure out who will take care of your kids when you die, which is what women tend to do [think of] - the worst case scenario.
What will it take for this to become a standard screening test?
It’s going to take a good guess five years before we will have irrefutable data that shows the superiority of CESM. It will take showing that it’s far superior to digital mammo alone, or in which population it’s superior at least and comparing it to MRI. Based on two years of data in Europe they are seeing a dramatic decrease in false positive rates. CESM is far more specific than MRI will ever be and it’s possibly just a smidgen less sensitive. That’s what they are seeing so far. It may or may not bear our when we have a large data pool to look at. If that seems to be the same story here, then I know we have a homerun on our hands.
Any advice or thoughts for other imaging centers considering this technology?
We have absolutely no hesitation or regret for implementing it. It has only brought an increased ability to diagnose cancers earlier and at more curable stages than we ever have before.
Craniocaudal view
Mediolateral oblique view
Images provided by GE, courtesy of Institut Gustave Roussy (IGR), Villejuif.
Advertisement
Related Content
Advertisement












Advertisement
Advertisement
Trending on Diagnostic Imaging
1
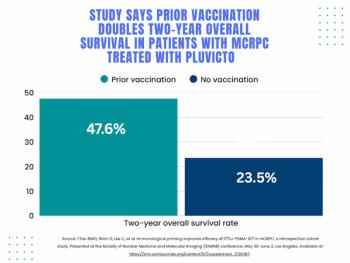
SNMMI: What Early Research Reveals About the Alpha-Emitting Radioconjugate ATNM-400 for Prostate Cancer
2
Mammography Study Shows Impact of AI-Powered Slab Reconstruction with DBT
3
Molecular Imaging in Focus: PSMA PET Radiotracers and Urinary Radioactivity: What Head-to-Head Prospective Multicenter Research Reveals
4
Molecular Imaging in Focus: SNMMI: Can a New Total Body PET Scanner Slash Scan Times and Bolster Sensitivity?
5