|Articles|March 14, 2012
Q&A: Taking on the Challenges of Imaging Prostate Cancer
Author(s)Diagnostic Imaging Staff
Radiology and imaging specialists Mukesh Harisinghani, MD, Frank Miller, MD, and David Casalino, MD, discuss an advanced image analysis technology, and the role of prostate MRI in cancer detection, localization, staging, treatment planning and serial monitoring.
Advertisement
Prostate cancer is the second most common form of cancer in men, yet diagnosing this condition still presents a challenge. Physicians have traditionally used the prostate-specific antigen (PSA) blood test to screen for prostate cancer. However, this diagnostic test may produce unclear results.
A new program is now being used at several sites to analyze MRI data with the goal of making test results easier to read and enabling physicians to pinpoint where a malignancy may be located in the prostate. By automatically generating visually intuitive colorized images that represent complex pharmacokinetic information and then overlaying it onto MRI images, physicians may be able to identify prostate cancers more accurately and with greater confidence.
In this Q&A, radiology and imaging specialists Mukesh Harisinghani, MD, Frank Miller, MD, and David Casalino, MD, discuss this advanced image analysis technology, and the role of prostate MRI in cancer detection, localization, staging, treatment planning and serial monitoring.
Can you discuss the current state of prostate cancer detection? How effective are current methods?
Casalino: The current methods of prostate cancer detection are digital rectal exam, serum PSA and biopsy. They all have their strengths and weaknesses and none are perfect. Some estimates report the digital rectal exam has a sensitivity of 50 percent and specificity of 80 percent, while PSA has a sensitivity of 72 percent and specificity of 93 percent. While a PSA level of 4 or higher is generally considered abnormal and concerning for prostate cancer, about 15 percent of "at risk" men with a PSA below 4 will have prostate cancer on biopsy. Men with an elevated PSA level in the borderline range - between 4 and 10 - have about a 25 percent chance of having prostate cancer. People are looking at percentage-free PSA, PSA velocity and PSA density to try and make it a better test, but there is still a ways to go.
Obviously biopsy of the prostate provides a means to make the diagnosis of prostate cancer, but according to some statistics, with a single session of prostate biopsies in a male with an elevated PSA, there is about a one third false-negative rate. The limitations of prostate biopsies relate to the limited number of biopsies. They are usually performed randomly and provide only very tiny pieces of tissue, so it is very possible that the biopsy will miss a tumor in the prostate or not accurately characterize a tumor that is discovered. Certainly DRE, PSA and biopsy do not provide perfect methods to screen for prostate cancer and make the diagnosis.
Harisinghani: Our ability to detect prostate cancer is getting better day by day. We are not as accurate as we would like to be. The main points in terms of detection are not only being able to detect the clinically significant disease in the prostate gland, and reliably locate the tumor, but also stage the cancer. With the techniques in MR, we are getting better, but its not 100 percent and there is room for improvement. That’s where MR is taking us now with all the new technological advances.
Why is prostate cancer detection so challenging?
Harisinghani: There are a few challenges we face. First, most prostate tumors are multifocal, which means that the tumor is not necessarily in one spot and it could be in more than one area. The other challenging part is the gland size varies among individuals. Someone could have a gland that is very small and someone else could have a gland that is very large. The tumor, depending on the size of the gland and the age of the patient, may not be as evident to the naked eye. So the multifocality and the varying shapes of the gland make it a challenge.
Another challenging problem is that some of the benign entities, like chronic inflammation in the prostate gland, can mimic tumors. By merely looking at the T2-weighted images, what you perceive as an area of abnormality may not necessarily be a tumor. So we need some other attributes, such as diffusion imaging and contrast enhanced MR that allows one to narrow the possibilities of entities that could mimic cancer.
How can MRI be used for prostate cancer detection?
Harisinghani: In terms of detection, there is a little bit of variability in use for MR. The three main questions you’re trying to answer for the treating urologist or radiation oncologist are: is there prostate cancer; where is it; and what are the multiple foci of disease in the gland and can we stage it locally. In terms of the first two questions, depending on the experience of the user and the technology you use, you are able to answer that question, although not to the extent the urologist would like us to. For the other question of staging, MR can be useful. Most centers use MR predominantly to stage the cancer. In the centers where you have reader experience and the necessary tools in terms of MR hardware and software, it is used for detection as well.
The other important point to remember is the treatment of prostate cancer is a moving target, so what was true a decade ago is changing. It’s not an aggressive disease like other cancers and it is common for patients to die from other causes rather than from prostate cancer itself.
Patients are willing to wait and not get treated because they don’t want to experience the side effects of treatments, such as sexual dysfunction and incontinence. There is a concept of surveillance or watchful waiting. Anytime you delve into something like that, it becomes absolutely critical that you are selecting the correct patient for that particular paradigm. If you put a patient on that surveillance protocol you want to be absolutely certain that, should there be any perceptible change, we should be able to catch it as soon as possible. This is another evolving indication or challenge remaining where MR is proving to be helpful. As the accuracy gets better, we keep getting better at it.
Miller: In the last several years, we’ve developed different techniques to allow us to see things better. We have better scanners. For example, at Northwestern we are using 3T scanners to see the prostate much better. The conventional images have improved over the years, but there are newer techniques, including diffusion-weighted imaging and perfusion-weighted or dynamic contrast enhanced imaging, which allows us to integrate multiparametric techniques to measure different features to provide functional imaging and assess the tumor’s vascularity.
Tell us about the technology you’ve been using to expand your detection ability.
Harisinghani: The role of MR in prostate cancer, albeit before detection or staging, requires a multiparametric approach - looking at the gland by more than one means on MR. On MR, there are multiple ways for looking at an area of interest. You can look at native tissue signature, T1 weighting or T2 weighting, you can look at diffusion properties, or you can look at enhancement properties with dynamic contrast enhancement. If you combine all these [areas] your accuracy gets better.
The three key components of the multiparametric approach are native tissue MR signature, T2 weighting, diffusion weighting and dynamic contrast enhancement. Contrast enhancement relies on contrast kinetics or how fast the tissue enhances. In a general term, that is referred to as dynamic contrast enhancement. Your naked eye is not able to pick up subtle differences that enhance differently. They may look very similar, but they are behaving very differently.
We’ve been using iCAD’s VividLook program, which is an excellent means to enhance the ability to distinguish two areas within the gland that behave differently after getting contrast. It’s able to get that information and color code it in a way that makes it very simple for us to look at and interpret. It makes our job easier from an interpretive point of view. By combining all the information together you are accurately able to localize the area of tumor. VividLook has definitely improved our accuracy. Our center was primarily relying on T2 weighting and diffusion weighting for detection of cancer. The challenge with these methods is that they are gray scale and it becomes a little difficult for our eyes to see the area of abnormality very well.
What information is obtained to enable you to determine localization, staging and treatment planning?
Casalino: Sites of prostate cancer typically show earlier, more intense enhancement and earlier, more rapid contrast washout compared with the normal prostate tissue. The dynamic enhancement information is captured in hundreds, occasionally thousands, of images. The key features may not be apparent on routine visual inspection. VividLook performs complex analyses of the dynamic enhancement data, colorizes the important features, and directs your eyes toward the areas most concerning for cancer.
An important concept in radiology is diagnostic confidence. When we have a patient with a positive biopsy for cancer and we want to stage the tumor and see if there are other sites of tumor that were not biopsied, we want to try to do it with as much confidence as possible. VividLook has improved our diagnostic confidence. On a single computer screen we typically link six different MR sequences so we can accurately correlate the T2-weighted imaging, the diffusion-weighted imaging, and the dynamic contrast enhanced imaging and data analyses to identify areas likely to be cancer. Needless to say, in someone who has a cancer and we want to stage it, to be able to correlate all three of those methods and to be able to pinpoint a specific site of abnormality across the board improves our confidence in identifying it as a likely site of cancer.
Where do you go from here with progress in the next five to 10 years?
Miller: We need to continue to do multi-institutional studies to confirm that the technique is working well, with the imaging findings correlating with the pathology findings. It is important to recognize that prostate cancer tends to be small and multifocal, so it can be hard to see. Other things people are considering are labeled agents that are taken up directly by the tumor for imaging and eventually therapy.
Casalino: There is still debate as to which analyses from the dynamic enhancement images are the best, so that’s an area of research - determining which of these parameters or combinations of parameters are going to be most helpful. There is data that suggests that how much restriction a tumor shows on diffusion-weighted imaging correlates with the aggressiveness of the tumor. An exam that could reliably differentiate a nonaggressive cancer from a highly aggressive cancer could have tremendous impact on how a patient is managed.
For example, if a test showed that a particular prostate cancer was not aggressive, watchful waiting, or active surveillance, might be the best approach for that patient, whereas another patient with a similar tumor in every other way but showing aggressive features might benefit from surgery or radiation therapy sooner rather than later.
The implications here are far reaching because prostate cancer is so common a disease, and there are many different factors that go into managing each individual patient. I am hopeful that MR of the prostate using current and future techniques will prove to be increasingly helpful in managing patients with prostate disease.
Mukesh Harisinghani, MD, is associate professor of radiology at Harvard Medical School and associate radiologist and director of abdominal imaging and intervention at Massachusetts General Hospital. Frank Miller, MD, and David Casalino, MD, are professors of radiology at Northwestern University Feinberg School of Medicine in Chicago, where Miller is also the chief of the Body Imaging Section and director of MR Imaging and Casalino is chief of Genitourinary Imaging.
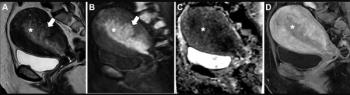
T-2 weighted MR image versus one colorized by VividLook. Images courtesy iCAD.
Advertisement
Related Content
Advertisement












Advertisement
Advertisement
Trending on Diagnostic Imaging
1
Can Contrast-Enhanced Mammography Improve Breast Cancer Staging?: Nine Takeaways from a New Literature Review
2
Breast Cancer Screening: Where Things Stand
3
What Does the Future Hold for Nuclear Medicine?
4
New CCTA Study Suggests that Current Plaque is the Key Biomarker for Assessing MACE Risk
5