
Blog|Articles|November 27, 2023
Questioning the Burgeoning Boilerplate in Radiology
Author(s)Eric Postal, MD
Excess verbiage, at the behest of non-clinical interlopers, continues to pervade radiology reports.
Advertisement
Teleradiology can be a challenging thing to explain to people. I don’t even try to convey the technical stuff. It is tricky enough to describe the logistics of reading for states A, B, and C while living in D but then shifting to coverage for X, Y, and Z while remaining in D.
I am not talking about how my screens can receive images and transmit reports hither and yon, because most people understand that from their own Internet usage. What is less intuitive is the often non-sensical difference in regulation between one state and another.
People reasonably expect health care to be a scientific thing. There aren’t substantial differences in human biology or CT scanners between, say, Florida and Maine. Why on Earth should it matter where my cases originate? Further, even if it is only on a subconscious level, folks might well be concerned about whether their particular state is regulating things well or in a way that degrades the quality/efficiency of the health care they are likely to get.
It doesn’t put them at ease when I tell them that certain states, for instance, require all their licensed physicians to undergo a certain amount of opioid-related CME during each licensing period even if said physicians, like myself, never prescribe any. Why, they might wonder, aren’t radiologists directed to spend those valuable hours of CME on something more, you know, radiological?
One quirk about my particular situation is that, even though I have lived in New York ever since med school, I haven’t actually read any cases from N.Y. in the past few years. I kept my N.Y. license, since I think it’s required while I read from there, but the last time I read for any facilities within the state was back in 2018. Subsequently, I have only read for facilities in Pennsylvania.
Beginning my new gig about three weeks ago was a virtual homecoming since I was once again reading for a couple of facilities in my home state. One of the first orders of business was therefore to get me up to speed on all of the regulatory nonsense here that hadn’t been in effect back in 2018. (If it was, my employer back then wasn’t aware of it or enforcing it. That happens a lot when you have excessively complex rules that are constantly changing.)
I pause to mention that, in this context, I use “regulatory” as a catch-all term for third parties who interfere with my medical practice. That includes not only appointed regulators from various levels of government, but also elected officials who choose to stick their noses into health care and insurance entities whose control of purse strings effectively gives them just as much power as any politico.
Let me reiterate that last point. If an insurance company threatens that it won’t pay you for your work because you didn’t dictate “Mother, may I” or “Simon says” in your report, you are just as likely to comply as if a bureaucrat mandated that verbiage. The insurance company’s power over you trumps anything you might have learned in med school, post-grad training, or however many years of your own experience.
(Editor’s note: For related content, see “
Fortunately, there wasn’t all that much new stuff for me to pick up. One item was a statement on all CT reports listing radiation dosage and number of CTs within the past 12 months. That routinely adds a paragraph to every dictation. Another was inclusion of bladder volumes, pre/post-void, on all pelvic ultrasounds even if the referrer was following fibroids and had zero interest in the urinary tract.
None of this stuff derails my day. I remember it easily enough and can incorporate it into my dictation macros. I couldn’t tell you the last time I had to make an addendum on account of having forgotten such things. I know other rads have had more trouble in that regard.
I used to get a little more worked up. How dare these non-physicians insert themselves into health-care relationships that should exclusively be between docs and their patients! These people never attended a day of medical school, probably couldn’t get in if they tried, and are trying to practice medicine without a license. They impose rules simply because they can. Maybe they think they can brag about it in their next election or simply expect to improve their profit margins.
Of course, I knew I couldn’t do anything about it so there was only so fired up I was going to get. My biggest peeve about the situation was — and remains — the addition of meaningless fluff to an already bloated medical record. This is stuff that is of absolutely zero help to the patient and various personnel trying to care for him or her.
For example, consider the new to me paragraph about radiation dosage and number of recent CTs. Does anybody seriously think a typical referrer is going to see that and think, “Gosh! I had better not scan this guy again” or, for that matter, even read the boilerplate? Chances are, seeing it in every single CT report he or she receives, the radiologist will likely skip over it just as much as he or she does the required blurb about how much contrast got injected per study.
There are plenty of other reasons why rads are justifiably irked when interlopers mess with our work. One reason doesn’t get as much attention. For a lot of the folks reading our reports (referrers, other clinicians getting involved in their patients’ care, the patients themselves, etc.), the assumption is that any/all excess verbiage can be blamed on the radiologist. As far as they can tell, we are the ones cluttering their documents with useless boilerplate. Maybe they even think we are somehow doing it for personal gain.
There is another thing that unhelpfully flies under the radar. The systems allowing our reports to be bloated like this are one-way valves. The various inroads these regulators have created can indefinitely be used to pump more fluff in, but there is no mechanism for extracting any of it. Rads (or the professional organizations supposedly representing us) never collectively push back and get any of these report requirements undone.
That is not a blanket accusation of our being lazy or ineffectual. It is pragmatism. Conduct a little thought experiment. Suppose we gather vast amounts of data showing that, despite a decade of radiation dosage reporting, no significant reduction of patient exposure has occurred. The paragraphs we are all dutifully including in our CT interpretations are demonstrably useless. We propose they no longer be required.
Do you think the paper pushers who forced this requirement on us would say “Yep, you’re right! We take it back” or is it more likely they would say that further study was needed before taking any action? I bet they would just insist that the boilerplate wasn’t worded strongly enough … and add to it.
Advertisement
Related Content
Advertisement










Advertisement
Advertisement
Trending on Diagnostic Imaging
1
New Study Shows Substantial Decline in CT Radiation Dosing for Adults Over the Past Decade
2
Study: AI Measurement of Coronary Inflammation from CT Scans Can Identify High CV Risk Patients with Low or Zero CAC Scores
3
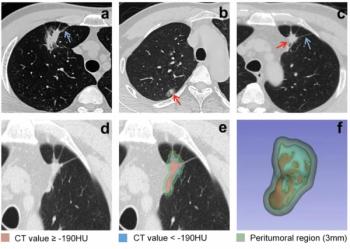
Can AI-Enabled Intratumoral CT Threshold Segmentation Help Predict Visceral Pleural Invasion in Lung Cancer Patients?
4
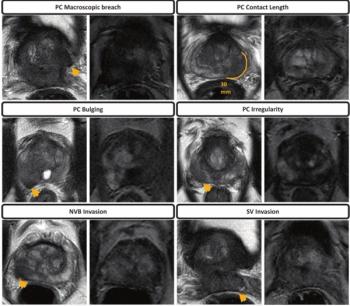
Does bpMRI Offer Similar Value to mpMRI in Detection of Extraprostatic Extension in Patients with PCa?
5