

|Articles|December 19, 2006
Report from RSNA: Breast MRI’s future depends on finding suitable indications
Continued concerns over breast MRI’s clinical cost-effectiveness can be fully addressed only if radiologists reach consensus on appropriate indications and development of standard protocols, according to New York-based researchers.
Advertisement
Continued concerns over breast MRI's clinical cost-effectiveness can be fully addressed only if radiologists reach consensus on appropriate indications and development of standard protocols, according to New York-based researchers.
Acceptance of breast MRI is being limited by cost issues, variability of equipment, lack of clarity over the technique and interpretation criteria, inability to reliably detect microcalcifications and ductal carcinoma in situ, and a higher false-positive rate than mammography.
MR-guided biopsies are still not widely available outside of academic institutions and tertiary-care centers, said Dr. Kristina Siddall, a radiologist in the department of imaging sciences at the University of Rochester Medical Center, in an educational exhibit at the 2006 RSNA meeting.
The American College of Radiology is developing criteria for individual program accreditation that addresses many of these concerns. As the list of appropriate indications is solidified, radiologists and surgeons will gain a better understanding of how best to use breast MRI, she said.
Breast MRI is most commonly used for evaluating patients with a known cancer. Accepted indications include the following:
- defining tumor size, extent, multicentricity, and multifocality
- screening the contralateral breast for cancer
- following treatment, determining response to chemotherapy, residual tumor after surgery, and possible tumor recurrence
Evaluation for occult breast primary tumor in the setting of axillary node metastasis is a less common but widely accepted indication.
"High-risk patients with a strong family history of cancer are also candidates for breast MR, and criteria for categorizing patients as high risk are evolving," Siddall said.
Protocol and indication differences have limited the reproducibility of research results, and technical factors such as motion artifacts, incomplete fat suppression, and sequence selection have affected the accuracy of individual studies. In patients with follow-up MR examinations, the time of menstrual cycle has added another variable.
Patient selection criteria have also directly influenced the scientific data. In a patient population with a low suspicion of disease, for example, the sensitivity of breast MRI is likely to lead to several false-positive findings and biopsies.
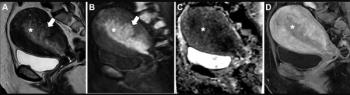
During the past 18 months, the Rochester group carried out breast exams on over 100 patients using a GE Signa 1.5T MR system and dedicated breast coil. A three-plane T1-weighted localizing sequence was followed by a series of sagittal sequences of both breasts. For adequate assessment of tissue vascularity, most exams required contrast, excluding breast implant evaluations for leakage and rupture.
The team obtained three postcontrast images, spaced at 60 to 90-second intervals after IV administration of 15 or 20 mL of a gadolinium-based contrast agent. Postprocessing entails a subtraction technique and generation of a maximum intensity projection from the first contrast-enhanced T1-weighted fat-suppressed image.
Siddall gave 10 reasons for ordering a breast MR exam:
- find out extent of disease (staging) in ductal carcinoma
- discover extent of disease (staging) in lobular carcinoma
- assess high-risk patients
- evaluate response to chemotherapy
- shed light on residual tumors
- assess tumor recurrence
- engage in problem solving/clarify inconclusive conventional imaging
- evaluate implant
- plan biopsy
- follow axillary lymph node malignancy or adenocarcinoma of unknown primary
For more online information, visit Diagnostic Imaging's
Advertisement
Related Content
Advertisement











Advertisement
Advertisement
Trending on Diagnostic Imaging
1
AI in Radiology: Emerging Trends, Current Obstacles and Future Directions
2
FDA Clears AI-Enabled Ultrasound for High-Volume Clinical Settings
3
Canon Medical Unveils Advances in AI-Enabled CT Software
4
Study Says Use of 18F-flotufolastat PET/MRI May Reduce Prostate Biopsies by More Than 50 Percent
5