
|Articles|May 1, 2007
Speech recognition technology speeds, simplifies report access
Author(s)Keith Grant, MD
Speech recognition technology can be integrated with most electronic medical record applications for rapid report creation. Searches, queries, and form filling are faster to perform by voice than using a keyboard.
Advertisement
Speech recognition technology can be integrated with most electronic medical record applications for rapid report creation. Searches, queries, and form filling are faster to perform by voice than using a keyboard. Hardware advances and improvements in the technology itself have brought the cost of ownership to an affordable level. Like any technology, however, deployment of a speech recognition program should be planned carefully to achieve full benefit from the software.
Clatterbridge Centre for Oncology is one of the U.K.'s largest cancer facilities. Speech recognition is now customized within CCO diagnostic imaging department to meet our needs, and the medical imaging reporting process has been streamlined. Our experience of implementing digital dictation and speech recognition may be useful to other hospitals that are interested in the technology.
The CCO diagnostic imaging department sees approximately 11,000 patients annually. It has a RIS and is working within the U.K. Connecting for Health program to implement a PACS. The system went live in March. Pre- and post-therapy examinations may involve x-ray, ultrasound, CT, nuclear medicine, and/or MRI. Medical imaging reports generated from these examinations provide the basis for clinical decisions. The department consequently decided to cut reporting turnaround times by integrating speech recognition with the departmental RIS.
CCO policy dictates that all reports are ready for verification within 24 hours of an imaging examination being performed. The last audit carried out prior to implementation of digital dictation and speech recognition showed that this target was not being met. Only one out of four MRI reports met this deadline, while just 11% of all x-ray reports were available within 24 hours.
Radiologists at CCO previously dictated onto cassette tapes. They now dictate directly into a patient's file, and the system adds corresponding patient information from the RIS. The final report is automatically stored in the RIS with the patient's exam history, improving security of patient data. Tapes with patient information are no longer in transit around the hospital, and paper reports do not need to be printed. Reports may be retrieved anywhere on the network using the correct authorization. Paper reports are printed because other users outside of radiology do not have access to the RIS; this function is going live with order communications this year.
Dictations that are required urgently can be accessed quickly. Staff members no longer have to spend valuable time finding and listening to previous dictations. Although CCO has no emergency department, procedures are in place for fast-track reporting of certain cases. For instance, emergency cord compressions films will be placed in front of the radiologist to report immediately.
A recent CCO audit found that 76% of all MRI reports are now available within 24 hours. X-ray reports showed the most dramatic improvement, although report turnaround for all modalities is now closer to the sub-24-hour goal (Table 1). Timely access to accurate imaging reports enables our clinicians to make informed decisions more quickly, while prompt availability of medical information prevents delays in treatment for patients.
IMPLEMENTATION ISSUES
The move from dictation onto tapes to speech-enabled reporting was a necessary part of the department's digitalization. This was performed in two consecutive steps. The department first upgraded digital dictation technology to speech recognition (SpeechMagic, Philips) within the RIS. The department went live with Philips digital recording, but secretaries still typed the report. The second stage enabled voice recognition, and the secretaries corrected/edited the dictated report. The system was then adapted to recognize text in line with specific reporting guidelines.
One major issue during the planning phase was motivating the departments' secretaries. The diagnostic imaging department has two full-time and one part-time secretary. Plans to implement digital dictation and speech recognition were met with uncertainty because the secretaries believed that a cost-cutting exercise might also mean staff cuts. This proved not to be the case, although the nature of their jobs changed. Secretaries now spend less time typing reports.
Radiologists also had to increase their IT skills, owing to the integration of speech recognition with the RIS. One radiologist initially resisted moving from tape to digital as he feared a potential system breakdown. Practicing with speech recognition in a training environment raised his confidence in the system before making the transition to digital recording. This initial onscreen training usually takes about 15 minutes. Users who have completed the training screens can then dictate real reports in a live environment.
Our speech recognition software was customized to fit medical reporting guidelines to ensure report consistency. Several radiologists use the system to generate medical imaging reports on a daily basis. Users include permanent CCO staff and specialist registrars who are trained on the system while rotating through the department. The training functionality allows temporary staff to create medical reports in the same way as permanent staff. The speech recognition system adapts their dictations according to departmental reporting guidelines. Radiologists do not have to change their dictation style because the system can interpret spoken words and correct the reports accordingly.
Diagnostic imaging staff members compiled a list of frequently used section headings to be added to the speech recognition system during implementation. The system now changes important terms according to the department's guidelines (Table 2). For example, if the doctor dictates "to conclude," the system will automatically insert the heading "conclusion." One radiologist may dictate "Dynamic CT scan," while another may use "CT scan dynamic." The speech recognition system will always change the spoken text into the preferred format.
Professionals are often hesitant to change their usual way of working. User acceptance of a new medical technology is consequently crucial to successful deployment. Customizing the speech recognition system to a department's needs significantly raises user acceptance. The disadvantage of customization lies in the time needed to install and integrate the speech recognition system. IT administrators, trainers, and secretaries were all involved in the customization process. The additional time and effort required for system customization did not affect radiologists.
UP AND RUNNING
The initial recognition level of our speech recognition technology was high. This allowed radiologists to begin using the system quickly and to speak naturally, while the software recognized the required format. Following correction of a report, the system adapts the user's profile and the corresponding acoustic reference files automatically to improve recognition accuracy. Once a radiologist uses an unknown word, such as the name of a new contrast agent, a RIS administrator will add that word to the radiologist's profile. Using the ConText Adaptation facility, the administrator can also decide to make the same vocabulary available to all radiologists within the department.
Radiologists and registrars may now choose whether to correct the recognized documents themselves or send the file to a secretary for formatting and completion. Doctors no longer have to search for the dictation device and blank cassette, dictate reports, and then physically deliver the tape to the secretary. The new system automatically routes files to the medical secretaries. A job list shows the transcription status so the doctor always knows when to expect a document for verification.
The display of all pending dictations on the job list allows the secretarial team to support one another and avoid backlogs. This results in much less pressure on individuals during holidays or illnesses. The team can also be supported easily by temporary staff. New secretaries can start working with minimal training because the system already recognizes medical terms used in dictation. The number of reporting errors has decreased thanks to the system's accuracy.
Secretaries are also less likely to suffer from wrist strain because repetitive key strokes have been eliminated. They now only have to listen to a report and make a few corrections. The reduced typing volume has allowed secretaries to spend at least two more hours a day on patient-oriented and administrative tasks, which has involved learning new skills. Job satisfaction has consequently increased.
RECOMMENDATIONS
Our experience has allowed us to develop several recommendations that might be useful for others who are introducing a speech recognition system.
It is vital to involve all staff from the start, acknowledging their fears and involving them in the introduction of speech recognition technology. Allowing clinicians to practice with the speech recognition system before it is installed in the department can raise confidence and aid acceptance of the new technology.
Not all speech recognition systems give radiologists the choice of dictating, correcting, and verifying reports themselves.
We recommend considering this feature, which can reduce report turnaround times further in an emergency or prevent backlogs if no secretary is available.
Speech recognition should be integrated in the departmental RIS or PACS to increase workflow efficiency and patient data security. It is not obligatory to customize the technology to the department's needs, but this does help achieve the full benefits of speech recognition.
Bibliography
- Borowitz SM. Computer-based speech recognition as an alternative to medical transcription. JAMIA 2001;8(1):101-102.
- Devine EG, Gaehde SA, Curtis AC. Comparative evaluation of three continuous speech recognition software packages in the generation of medical reports. JAMIA 2000;7(5):462-468.
- Houston JD, Rupp FW. Experience with implementation of a radiology speech recognition system. J Digit Imaging 2000;13(3):124-128.
- Mehta A, McLoud C. Voice recognition. J Thorac Imaging 2003;18(3):178-182.
- Mohr DN, Turner DW, Pond GR, et al. Speech recognition as a transcription aid: a randomized comparison with standard transcription. JAMIA 2003;10(1):85-93.
Ms. Aspinall is a clinical electronic patient records trainer, and Dr. Grant is the clinical director of diagnostic imaging, both at Clatterbridge Centre for Oncology in Bebington, Wirral, U.K.
Advertisement
Related Content
Advertisement













Advertisement
Advertisement
Trending on Diagnostic Imaging
1
Can AI Enhance Non-Contrast and Contrast-Enhanced CT Detection of Pancreatic Cancer?
2
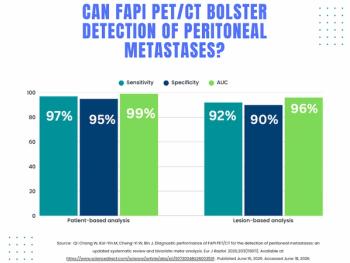
What a Meta-Analysis Reveals About FAPI PET/CT for Detection of Peritoneal Metastases
3
Emerging PET Radiotracer May Enhance Detection of Small Metastases in Patients with Advanced Melanoma
4
Can Photon-Counting CT Provide Timely Clarity After Mechanical Thrombectomy?
5