
|Articles|February 1, 2009
Worldwide travel triggers spreadof parasitic CNS infections
Author(s)María Navallas, MD
Vaccines, antibiotics, and other therapeuticagents have kept most infectious diseasesunder control in industrialized nations. Indeveloping countries, however, infectious diseaseshave been harder to contain.
Advertisement
Vaccines, antibiotics, and other therapeutic agents have kept most infectious diseases under control in industrialized nations. In developing countries, however, infectious diseases have been harder to contain. The current upsurge in immigration and global travel is now leading to the introduction of infections into industrialized countries where they were previously almost nonexistent.1
Central nervous system infections remain a challenging problem. They are among the leading causes of death in underdeveloped countries. Patients present with a variety of clinical symptoms, and imaging plays a crucial role in the diagnosis, along with the patient’s history, host factors, physical examination, and laboratory analysis of cerebrospinal fluid. CNS infections are potentially treatable, but early detection, specific diagnosis, and prompt treatment are important to prevent permanent neurological deficit and/or spinal deformity.2
Hydatid disease is a zoonosis caused by the larval stage of the Echinococcus granulosus tapeworm and, rarely, the E multilocularis tapeworm. It is a significant health problem in underdeveloped areas where animal husbandry is common but no veterinary control exists. The liver is the most frequent site of involvement (75% of cases), followed by the lungs (15%). The CNS is affected in just 1% of cases.
The life cycle of E granulosus involves two hosts. The adult worm of the parasite lives in the small bowel of the definitive host, usually a dog. Eggs are released into the host’s intestine and excreted in the feces. Humans become infected by contact with a definitive host or by ingestion of contaminated water or vegetables. Cerebral infection is very uncommon and usually diagnosed during childhood. It accounts for only 2% of all intracranial masses, even in countries where hydatid disease is endemic. Cysts are usually located in the hemispheres, especially in the vascular territory of the middle cerebral artery.3
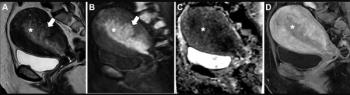
Imaging will show a single well-defined, smooth, thin-walled, spherical cystic mass with attenuation or signal intensity similar to that of cerebrospinal fluid. Mass effect can be observed, but there is no associated edema. There is no enhancement after contrast administration, and calcification is extremely rare.4 The cyst wall is usually seen as a rim of low signal intensity on both T1- and T2-weighted MRI. It is clearest on T2-weighted images owing to the contrast between the lowsignal- intensity cystic wall and the high-signal-intensity fluid content.5
Differential diagnoses include abscess, cystic astrocytoma, arachnoid cyst, and porencephalic cyst. The lack of surrounding edema and the marked mass effect make it easy to distinguish hydatid cysts from abscesses and cystic tumors. Hydatid cysts are spherical, unlike arachnoid and porencephalic cysts.6
Intracranial subarachnoid spaces are the second most commonly affected location in the CNS, though hydatid disease occurs far less frequently here (
Cysticercosis is the most common parasitic infection of the CNS in immunocompetent individuals and the most common cause of seizures in young patients in developing countries.8 Neurocysticercosis is being increasingly observed in nonendemic areas, thanks to migration and global travel.8 Infection can be traced back to the larval pork tapeworm, Taenia solium, and may involve almost any body tissue. The preferred sites of implantation are the brain (70% to 90% of all cases), muscles, skin, and eyes.9 Correct diagnosis is based on laboratory tests and imaging findings.9
Humans usually become infected by eating viable cysticercus larvae from pork meat. Infection can also occur after ingestion of embryonated Taenia eggs deposited on fecally contaminated food, though this path is rarer. Inflammatory reactions associated with the parasites’ dying process usually trigger disease symptoms.10 These will depend on the number, size, and location of cysts.
Neurocysticercosis may involve the subarachnoid space, brain parenchyma, ventricles, and spine.11 The most common location is the subarachnoid space (typically basal cisterns and deep within the sulci) where cysts may have a racemose form. Large cysts can produce CSF obstruction. The inflammatory reaction may cause adhesion of the adjacent gyral surfaces, leading to the mistaken impression that the cyst is intraparenchymal.12
Cortical areas and basal ganglia of the brain parenchyma are the second most common location. Intraventricular cysts can be seen here, too, especially in the aqueduct of Sylvius and the fourth ventricle. These lesions are usually solitary, pedunculated cysts that can migrate and produce acute obstructive hydrocephalus. Neurocysticercosis rarely involves other locations, such as the spinal cord.
Imaging findings vary with the stage of cyst development, which is a four-stage process. The initial vesicular period is typified by a thin-walled cyst. It is CSFlike on CT and MRI and will show a small, eccentric invagination developing along one cystic wall (scolex) associated with minimum inflammation. The scolex is best seen on proton-densityweighted images and may be obscured by high-signal-intensity cystic fluid on T2-weighted MRI.9
The colloidal stage is characterized by the parasite’s death. Symptoms usually appear at this point. Imaging will show an inflammatory reaction of the surrounding neural tissue with edema and ringlike enhancement of the cyst without a well-defined scolex. The severity of inflammatory response will depend on the host’s immune response.
The nodular or granular period occurs next, when fibrosis causes the cyst to collapse. Edema decreases, and the enhancement pattern becomes more annular and thicker, or nodular. The final residual stage describes the point when granulomatous lesions are shrunken, and small calcified nodules without mass effect are found. These nodules are hypointense on all MRI sequences (
Schistosomiasis is a helminthic disease endemic in the tropics and subtropics, especially in eastern Asia, South America, and Africa. It is the second most common human parasitic disease after malaria and is now being imported into temperate climates.13
Five species of flat worm can cause schistosomiasis: Schistosoma mansoni, S haematobium, S intercalatum, S japonicum, and S mekongi. The life cycle of Schistosoma is extremely complex. The freshwater snail releases Schistosoma cercariae into the water. The cercariae infect humans percutaneously and transform into schistosomula. These schistosomula migrate to the lungs and the liver where they mature into adult worms and form male-female pairs. They then descend to the mesenteric venous system and the venous plexus of the bladder where they begin to lay eggs. Some of the eggs are voided in urine, and others exit in feces. About 50% of the eggs become trapped in the body and release proteolytic enzymes that produce an eosinophilic inflammation and a granulomatous reaction.14
Schistosoma species ova can reach the CNS in two different ways. Eggs can be carried to the CNS through arterial or retrograde venous blood flow and may be deposited anywhere en route. Adult worms can also migrate abnormally and deposit the ova in situ.15
Neuroschistosomiasis is usually asymptomatic. Symptoms such as seizures and neurological focality are more frequent in young men. CT findings of cerebral schistosomiasis consist of single or multiple enhancing hyperdense lesions surrounded by low-density edema with an associated mass effect.16 MRI reveals a central linear enhancement surrounded by multiple enhancing punctate nodules. These are clustered in a masslike structure with arborized appearance. This finding seems to be a highly specific indicator of CNS schistosomiasis (
Definitive diagnosis requires a cerebral biopsy to prove the presence of eggs in the CNS. Pathology will depend on the intensity of infection and the host’s immune system. Patients may exhibit no reaction, limited inflammation, localized vasculitis, or, more frequently, tissular necrosis with granuloma formation. A favorable outcome depends on early diagnosis with immediate treatment.
A number of other less common parasitic infections also can affect the CNS. Trichinosis is best known for involving the muscles. Brain lesions are rare, but eosinophilic meningoencephalitis, vascular thrombi, and infarcts can be found. Paragonomiasis is characterized by a calcified mass and can simulate a neoplasm in the chronic stage. The most common, characteristic imaging finding in the early active stage is a conglomerate of ringlike enhancing lesions with surrounding edema in one cerebral hemisphere.17
Cerebral malaria has a predilection for the basal ganglia and the cortex. Hemorrhagic foci and cortical infarcts will be seen here. White matter lesions and brain swelling can also be detected. Trypanosomiasis is characterized by meningoencephalitis, cerebral edema, and petechial hemorrhage. CT findings characteristic of sparganosis include white matter hypoattenuation with adjacent ventricular dilatation, irregular or nodular enhancing lesions, and small punctate calcifications. Sparganosis can be mistaken for a neoplasm when it appears as a multicystic mass surrounded by edema.
Amebiasis is typified by meningoencephalitis or by solitary or multiple masses with punctate, nodular, or annular enhancement. Coenurosis is extremely rare. This condition may resemble cysticercosis but causes single lesions in the brain more often than cysticercosis does. Toxocara, Trichinella, Strongyloides, and Angiostrongylus typically cause meningoencephalitis. Focal brain lesions are rare.
Physicians diagnosing a tropical disease should ask these questions: Where has the patient traveled or where does he or she come from? What did he or she do there? What clinical features stand out? What are the principal imaging features? What would a local doctor think?
Cysticercosis is the most common CNS parasitic infection. A seizure associated with a focal lesion in the brain is most often due to cysticercosis in tropical or subtropical regions.8 Hydatid disease should be considered when a cystic lesion is identified in a patient who lives in or has come from an endemic area, especially if he or she has known hydatid disease elsewhere-for example, in the liver or lungs.
Central linear enhancement on MRI, surrounded by multiple enhancing punctate nodules forming an arborized pattern, is strongly suggestive of schistosomiasis. 15 The most efficient MR sequence for diagnosing subarachnoid spinal hydatid disease is 3D fast imaging with steady-state acquisition.
Advertisement
Related Content
Advertisement











Advertisement
Advertisement
Trending on Diagnostic Imaging
1
Can Contrast-Enhanced Mammography Improve Breast Cancer Staging?: Nine Takeaways from a New Literature Review
2
Breast Cancer Screening: Where Things Stand
3
What Does the Future Hold for Nuclear Medicine?
4
New CCTA Study Suggests that Current Plaque is the Key Biomarker for Assessing MACE Risk
5