
|Articles|February 7, 2006
Imaging strategies take on growing importance in ablation
Clear, effective imaging is vital to tumor ablation, but consensus on which imaging method to use when has been elusive. No imaging modality on its own is perfect, and what may work well in one situation will be ineffective in another.
Advertisement
Clear, effective imaging is vital to tumor ablation, but consensus on which imaging method to use when has been elusive. No imaging modality on its own is perfect, and what may work well in one situation will be ineffective in another.
"Imaging is playing an increasingly important role in guiding and monitoring ablation therapies," said Dr. Fred Lee, a professor of radiology at the University of Wisconsin Medical School. "I feel like I can put any size hole in any size tumor in any organ. My biggest challenge is knowing whether I've gotten the whole thing and whether I'm done with the procedure."
Dr. Fred Lee, a professor of radiology at the University of Wisconsin Medical School
Dr. Stephen Solomon of the Memorial Sloan-Kettering Cancer Center in New York City
ULTRASOUND
Ultrasound is one of the most effective real-time imaging methods currently in use, but it has significant drawbacks. Ultrasound cannot see temperature changes in a lesion but instead shows the bubble cloud caused by ablation, said Dr. William Lees, director of the Centre for Medical Imaging at University College Hospital in London. The bubble cloud obscures what is behind it, which may lead a physician to overestimate the area of final necrosis.
It can be difficult to find a lesion with ultrasound, and it's not easy to spot nearby critical structures, said Dr. Stephen Solomon of the Memorial Sloan-Kettering Cancer Center in New York City.
Some of those drawbacks can be countered by using contrast-enhanced ultrasound, according to Lees.
"It has transformed liver ultrasound, from the characterization of lesions to the detection of lesions, and it's very useful in RFA for checking the completeness of the ablation," he said. "We're using it pretty routinely - not in every case, but in most cases."
In the U.S., ultrasound contrast agents have not been licensed for use outside of the heart.
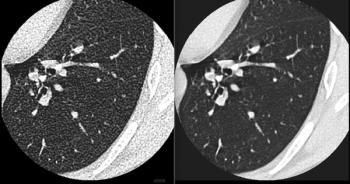
CT
CT can provide a good picture of the lesion and the surrounding structures, but it does not work as a real-time imaging method. In addition, there may be accessibility problems with the bore size of the scanner - probes protruding from the patient may be knocked out of place by the scanner itself.
New equipment is helping to ameliorate some of these difficulties, Solomon said. For example. semiflexible probes can be used in tight situations, and larger bore sizes make CT more accessible to both physician and patient.
In many cases, physicians can combine the best aspects of ultrasound and CT by fusing the two images together, he said.
"We do all of our ablations in the interventional CT suite," Lees said. "With ultrasound, we do an initial CT, then coregister the ultrasound system to the CT."
MR
MR may be one of the most controversial imaging methods for tumor ablation. Some physicians see it as the best method available, while others dismiss it as overhyped. Lee falls in the first camp.
"MRI might be the most natural guidance modality by giving us multiplanar imaging - rapid feedback of where our needle is in relation to the tumor in 3D - and the ability to monitor the results of the treatment, particularly by the use of thermal mapping," he said.
But access to MR tends to be limited, and its costs are high, so it hasn't gained wide acceptance as an imaging method for ablation.
Lees takes the opposite tack. He sees MR as too slow and considers the image quality it produces insufficient for use in tumor ablation.
"MRI is almost too powerful," Lees said. "You see lots of different things happening simultaneously. One thing is driving the signal up while another is driving the signal down, and you end up with a very complex set of sequences that are very hard to interpret. In my practice, CT with contrast gives you basically what you need to know, which is what is alive and what is dead."
PET/CT FUSION AND FOLLOW-UP IMAGING
Although PET plays a limited role in intraprocedural imaging, it can be useful both before and after a procedure, Solomon said. PET can identify areas of metabolic growth, while CT can target the structure of the lesion. When the two images area fused together, the composite can provide an early warning of tumor resurgence or new disease.
New tools and new opportunities to fuse existing imagine methods are opening up more ground for tumor ablation, and radiologists must rise to the challenge, according to Solomon.
"The focus for radiologists has always been on making the prettiest picture," he said. "As we tend toward image-guided interventions, we must shift that focus more toward making the most useful image, even if it includes many different aspects from other image modalities."
Advertisement
Related Content
Advertisement













Advertisement
Advertisement
Trending on Diagnostic Imaging
1
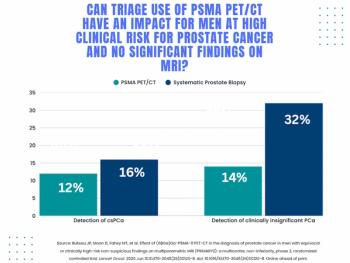
Study: PSMA PET/CT Reduces Biopsy Rate by Nearly 50 Percent for Men with Equivocal or Non-Suspicious Prostate mpMRI
2
Mammography Study: Can AI Detect Potential Breast Cancer Up to a Decade Prior to Diagnosis?
3
The Hidden Social Price of Remote Work in Radiology
4
Addressing Challenges in Radiology Reporting
5