
|Articles|January 1, 2009
- Diagnostic Imaging Vol 31 No 1
- Volume 31
- Issue 1
Focused ultrasound ablation offer prostate cancer option
Author(s)Clare Tempany, MD, Jalil Afnan, MD
Prostate cancer is a leading cause of cancer death inU.S. men, second only to lung cancer. During2008, an estimated 186,320 new cases of prostatecancer will be diagnosed in the U.S.
Advertisement
Prostate cancer is a leading cause of cancer death in U.S. men, second only to lung cancer. During 2008, an estimated 186,320 new cases of prostate cancer will be diagnosed in the U.S. Approximately one in six men will be diagnosed with and one in 34 will die of prostate cancer.1
Once a diagnosis is made, the extent or stage of the disease must be determined before treatment decisions are made. The most critical issue is whether the tumor is confined to the prostate gland itself or extends beyond.
Staging is based upon a combination of the clinical results of the prostate-specific antigen test and its subanalysis such as velocity and density, the Gleason score, a patient's age, imaging such as endorectal coil MRI, and family history.
Localized prostate cancer treatments range from the aggressive radical prostatectomy to active surveillance, or watchful waiting. Selection of treatment is based on a full evaluation of the risks and benefits of all treatment options within the context of the patient's situation. Chief treatment determinants are medical recommendations, patient preferences, and local expertise, including the availability of various treatments.
Major concerns include the possibility of successful treatment of the tumor and the extent of side effects. Given the extreme range of treatment options and concern about side effects, patients and their doctors are giving close scrutiny to new focal and/or minimally invasive treatments as possible alternatives.
These alternative focal treatment options differ from traditional approaches in that they do not treat the entire prostate gland as if it were uniformly filled with cancer. One major driver of alternative treatment approaches, or less than total gland treatment, is the desire to preserve the patient's quality of life. The side effects of traditional prostate surgery and radiation include incontinence, impotence, and rectal damage (from the radiation).
Traditional surgery always involves total gland removal, and radiation treatments deliver uniform doses of brachytherapy and external-beam radiation, for example, to the entire gland. The newer treatment of intensitymodulated radiation therapy (IMRT), however, allows for dose escalation to focal regions.
New radiation planning software now offers so-called dose-painting approaches to tailor dose delivery to only those predefined abnormal regions of the gland. These regions are most commonly MRI-defined. MR-guided brachytherapy, pioneered by D'Amico et al,2 was one of the first "sub-total gland" treatments established for prostate cancer. It uses MR images to outline a subregion of the gland, generally the peripheral zone of the gland as seen on T2-weighted MRI, to define the clinical target volume. Compared with radical prostatectomy, MR-guided brachytherapy is very successful in that it has led to similar outcomes and more favorable quality of life.3,4 Using other radiation approaches such as IMRT can minimize some side effects. Surgical approaches can also be modified to some degree using laproscopic or robotic techniques. These efforts are mainly directed at reducing perioperative morbidity and length of stay in the hospital, however, and early evidence suggests that they require significant expertise and can be associated with significant failure rates.5
Another alternative to conventional prostate treatment that has been in clinical use worldwide for many years is therapeutic ultrasound using focused acoustic energy to cause thermal coagulation deep within the prostate. Parts of the prostate gland can be ablated once a high-intensity ultrasound beam is localized to a small focal point, resulting in individual sonications causing thermal damage, or thermocoagulation. To control the ablation and minimize side effects, a clinician can regulate ultrasound power deposition and other parameters so as to ablate only the intended volume of tissue.
When focused acoustic energy is combined with MRI as the imaging guidance tool, the technique is known as MR-guided focused ultrasound surgery (MRgFUS), but when it is used with ultrasound, the technique is generally known as high-intensity focused ultrasound (HIFU). MR's critical advantage is its ability to provide MR thermometry to allow real-time feedback of therapeutic heating effects during treatment.
Early work on focused ultrasound was reported by Lynn et al, who offered an understanding of the biological effects of ultrasound at the cellular level,6 and the Fry brothers, who introduced HIFU applications in brain disease human trials.7 Focused ultrasound treatment of prostate cancer was first reported by Bihrle et al and Chapelon et al.8,9
TECHNICAL EXPERIENCE
Most prostate cancer patients who have undergone focused ultrasound therapy have been treated with one of two devices developed by EDAP TMS (Lyon, France) or Focus Surgery (Indianopolis).10-13 These devices use a small single-channel (i.e., fixed focused) transducer operating at approximately 3 to 4 MHz that is integrated within a rectal probe. The transducer is connected to a shaft within the probe that is coupled to a robotic positioning system. This allows the transducer and the focal point to be steered to the desired points within the prostate.
Also integrated within the rectal probe is an ultrasound imaging transducer used for treatment planning. Two approaches have been tested for HIFU: In one, the imaging probe is advanced into the rectum during treatment planning and then retracted during treatment (see bottom illustration, page 24); in the other, simultaneous imaging and therapy are possible when either the same transducer alternates between imaging and therapy modes or an imaging transducer is located in the center of the treatment transducer (see top illustration, page 24).
The entire probe is surrounded by a thin plastic or latex condom filled with temperature-controlled degassed water. This serves multiple purposes during the treatment, including providing acoustic coupling for the ultrasound beam (so beam does not propagate into the air), chilling the rectal wall to prevent unwanted thermal damage, and creating pressure to restrict motion of the rectum and prostate.
During the ultrasound exposures ("sonications") in HIFU, standard b-mode ultrasound imaging does not accurately depict thermal changes within the heated zone.14 Hyperintense regions may appear during each sonication in the focal zone, however, presumably due to bubble formation (cavitation) possibly induced by boiling or the intense negative pressures associated with highintensity ultrasound exposures. These regions, while not necessarily predictive of the resulting thermal lesions, provide some level of feedback to the operator.
This lack of effective image guidance is a major limitation of focused ultrasound and can result in undertreatment of the gland. Multiple research groups have investigated ultrasound-based thermometry methods with some promising results, however.15-18 Others have investigated using elastography methods to detect thermal coagulation. 19 These methods, which are sensitive to mechanical tissue properties, have shown promise in delineating thermally coagulated zones that are stiffer than normal tissue. Other researchers have investigated the use of mechanical tissue disintegration as an alternative to thermal ablation. 20 Here, very short, intense, focused ultrasound pulses are delivered to mechanically break up tissue in the focal zone. Ultrasound imaging has shown promise in detecting these mechanically ablated zones.21 The only available imaging method that provides accurate quantitative temperature mapping is MRI. The water proton resonant frequency depends linearly on temperature over the range of temperatures used in thermal ablation22 that can be rapidly measured using standard imaging methods.23 MRI's temperature sensitivity also appears to be insensitive to tissue type24 and does not alter with heat-induced tissue changes.25 Through its temperature measurements, one can verify the focal point position before any thermal damage occurs, predict the extent of thermal necrosis, and monitor surrounding tissue for heating before damage occurs.
In addition to the problem of image feedback with currently available focused ultrasound devices, the therapy is limited by long treatment times and difficulty in focusing at sufficient depths to cover the entire prostate gland. To reduce these problems, one approach is to decrease the volume of the prostate before focused ultrasound, using transurethral resection of the prostate (TURP). The most common surgical procedure for treating benign prostatic hyperplasia, TURP involves the insertion of a cystoscope through the penis and urethra into the prostate gland where a special cutting instrument is pushed through the cystoscope to remove the gland in pieces.
Another approach has been to use a two-sided transducer with two focal lengths to target different depths. Other researchers have investigated using phased-array transducers to extend the range of the focal point.26-28 Such arrays consist of multiple transducers with individual driving systems. By manipulating the phase of the individual driving systems, one can electronically steer the focal point and extend the treatable range of the system.
Such arrays can also be used to increase the total focal volume either by steering the beam to different locations during each sonication or by creating multiple foci simultaneously. Steering the beam to cover the entire gland requires many hundreds of transducer elements. A simple approach to increase the focal volume, which has been successfully tested with the prostate, is using a so-called split-focus transducer that, once implanted, can produce four focal spots simultaneously with only four transducer elements.29
Combining phased arrays with the imaging and thermometry capabilities of MRI can potentially address the limitations of current prostate-focused ultrasound devices. Under MRI guidance, transrectal prostate phased-array treatment probes have been tested in animal trials.27,28 Recently, InSightec (Haifa, Israel) constructed an advanced prototype clinical system that contains a 1000- element phased-array transducer integrated into either a 1.5T or 3T clinical MRI unit that is being tested in animal trials at several institutions. Examples of temperature mapping during sonication with this device, used along with MRI and histology of the ablated volume, are shown in Figure 1.
Compared with a transrectal approach, alternative ultrasound treatment strategies have also been proposed that may have some superior advantages. Transurethral ultrasound probes, for example, have been suggested and tested in animal trials.30,31 These devices produce a narrow heated beam that radiates outward from the prostate. By controlling the heating duration and rotating the device, the operator may ablate the entire gland in a fairly short period of time. By dividing the transducer into several elements along the direction of the probe and monitoring heat progression with MR thermometry, one can contour the treatment to the prostate anatomy through individual control of the elements.
Similar to radiofrequency or microwave devices, other probes have been tested that are inserted interstitially into the prostate.32 Ultrasound probes have advantages over other interstitial probes, however, in their ability to direct energy in a desired location with certain penetration capabilities. Transperineal approaches have also been suggested.33
CLINICAL EXPERIENCE
When applied to prostate cancer, the aim of HIFU is to cure most patients. The optimal pretreatment patient profile is localized disease with clinical stage T1-2, Nx to N0, M0, PSA score < 10, Gleason score < 7, and prostate gland volume of less than 40 cc. Other patients who might benefit from HIFU are those with a comorbidity preventing major surgery, age greater than 70 years, remaining life expectancy of less than 10 years, and recurrence of disease following radiation or brachytherapy.34
Contraindications to HIFU therapy include a large prostate, the presence of calcification within the prostate, disseminated disease, and anatomical or pathological limitations to the placement of the endorectal device. Neo-adjuvant treatment to reduce prostate size may be employed, either surgically via TURP or chemically through androgen suppression with a combination of gonadotropin-releasing hormone agonists, nonsteroidal anti-androgens, and 5-a reductase inhibitors.35
HIFU can be performed under spinal or general anesthesia and done on an outpatient basis.
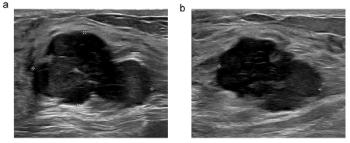
Depending on the number of areas that require treatment and the extent of disease, a single session lasts several hours. Protocols are based on whether treatment is an initial session or repeat procedure, with prior treatments including radiation therapy. Following placement of the device, the use of ultrasound for real-time registration follows. The differences between prostate ultrasound and MRI for visualization of the prostate and its substructures are seen in Figure 2. The HIFU operator adjusts power output according to evolving conditions within the prostate and the proximity of the focus to neighboring structures, including the neurovascular bundle and rectal wall.
SUCCESSFUL TREATMENT
Successful treatment is defined by radiological, pathological, and biochemical markers of disease. Over a decade ago, Madersbacher et al presented details of successful HIFU treatment.36 Subsequent trials have reinforced findings that HIFU can be successful, evidenced by approximately 54% to 77% of patients being free of disease five years after treatment. Blana et al identified greater than 75% patients as disease-free; however, a significant proportion of these patients had received neo-adjuvant hormonal therapy that may have biased the results.10
Misrai et al also found a possible effect of hormonal therapy on successful outcome. In that work, involving long-term results of HIFU, patients received treatment based on the stratification proposed by D'Amico et al, meaning they were grouped as low-risk, intermediate-risk, or high-risk patients. The high-risk population, in which no patient had previously undergone hormonal therapy, was the population most likely to develop recurrence, characterized by biochemical failure.11
Adverse effects from HIFU, as published by Thuroff et al,12 include urinary retention (8.6% patients), stress incontinence (13.1%), bladder outlet obstruction (3.6%), urinary tract infection (13.8%), and urethrorectal fistula (1.2%).
Other studies have identified greater degrees of impotence, at approximately 50% of patients.37 These patients, however, received multiple HIFU sessions. These adverse effects are results from older work; newer improved devices reduce these effects.
MR as the imaging guidance method will offer a significant advantage over ultrasound by reducing adverse effects, as it more accurately monitors temperature in the volume of ablation to better allow for real-time adjustment of energy to the device.
As seen from study results to date, HIFU for prostate cancer is a useful and successful treatment option. The best results for HIFU most likely depend on a wellchosen patient population and may incorporate the use of adjuvant or neo-adjuvant hormonal therapy.
Based upon prior research and clinical experience with the treatment with uterine fibroids,38 our group and others are investigating MRgFUS as a potential therapeutic approach for prostate cancer. Significant advantages result when thermal energy deposition is combined with direct MR guidance, coupled with real-time MR thermometry. Clearly, the imaging and engineering challenges require safe and effective delivery of the ultrasound beam in the MR environment.
In summary, as the device technology evolves, so does MR imaging of the prostate. With the shift to 3T endorectal coil MR imaging, the ability to select and monitor targets and surrounding tissues will continue to improve. We believe that the combination of these two research initiatives will result in the development of a unique and exciting treatment option for men with prostate cancer.
Articles in this issue
over 17 years ago
When the RSNA throws the book at us, we read it allover 17 years ago
California blamesoperator errorfor CT incidentover 17 years ago
Is this radiology's best connected couple?over 17 years ago
Iso-osmolar agent showshigher renal failure rateover 17 years ago
CMS hesitates to approvePET for cancer despite dataover 17 years ago
Chest CT assists follow-upof head and neck cancerover 17 years ago
Economic woes affect attendanceover 17 years ago
Expertise with MSCT-CA takes timeover 17 years ago
Illegal patient info sneaks into PowerPoint filesover 17 years ago
Moolah getsreports flyingout the doorAdvertisement
Related Content
Advertisement













Advertisement
Advertisement
Trending on Diagnostic Imaging
1
Observations and Reflections from the 2026 SNMMI Conference: An Interview with Jeremie Calais, MD, PhD
2
FDA Clears Emerging AI Segmentation Module for Brain MRI
3
Aidoc’s First Read X-Ray Reporting Software Gets FDA’s Breakthrough Device Designation
4
New AI-Agnostic Radiology Reporting Platform Facilitates Ease of Integration into Existing Systems
5