












Opposition to AI in Mammography; Alzheimer's Disease and Vascular Dysfunction; Clear & Present Danger for The Match; Trends & Innovations in Breast Imaging
Opposition to AI in Mammography; Alzheimer's Disease and Vascular Dysfunction; Clear & Present Danger for The Match; Trends & Innovations in Breast Imaging
Delays in the diagnosis and treatment of breast cancer have led to the creation of multidisciplinary recommendations for breast cancer care during the COVID-19 pandemic.
More than three-quarters of women prefer a radiologist to be involved with reading their screening studies.

Dual-Energy CT's Impact in the Emergency Department; Mass Casualty Planning; Language Barriers to Mammography for Spanish-Only Speakers; Improving the Patient Experience for Mammography During the Pandemic

Identifying a patient’s preferred method of communication can open the door for optimal, respectful patient care.
Women who have limited English proficiency have significantly lower rates of undergoing this exam.
Synthetic mammography performed equally as well to digital mammography with less radiation exposure.

Breast imagers could be among the most highly burned out sub-specialists, but there are ways to reduce the work fatigue.

PET/MRI vs. PET/CT; Abdominal CT and COVID-19; Chest MRI vs Chest CT; Expert Interpretations of Endometriosis; and Delayed Breast Cancer Treatments for African American Women
In a one-on-one conversation, Murray Rebner, M.D., past president of the Society of Breast Imaging, discusses how current screening guidelines overlook these women and what that means for radiologists.
Radiation, alongside age and socioeconomic status, is associated with longer diagnosis-to-treatment timelines.
Time of day can affect how well a radiologist can identify and diagnose normal lesions.

Rethinking CMR during COVID-19; Abdominal Imaging and COVID-19; Mental Health Impacts of COVID-19; African American and Lung Cancer Screening; Plus, African American Women and Disadvantages in Breast Cancer Screening
Women treated with both surgery and radiotherapy for ductal carcinoma in situ fared best.
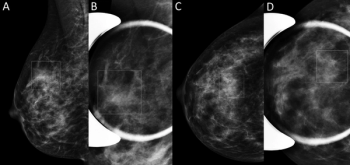
Combining DBT and synthetic mammography can mean less follow-up imaging for women with non-dense breasts – but not necessarily for women with dense tissue.

A model that includes mammographic features, lifestyle factors, and genetic-based risk prediction scores can effectively pinpoint which women will likely receive an interval cancer diagnosis.
Researchers endeavor to make thermography a strong supplemental tool to mammography.

What’s keeping women from mammography, and what imaging professionals can do to help.

This AI tool is designed to work independently, dividing scans between those that need no radiologist assessment and those that require further interpretation.

Artificial intelligence equivalency in breast cancer screening; diffusion-weighted imaging and breast MRI; CT patterns for EVALI; Emergency Department and CT Scan Declines with COVID-19; and Thoracic Imaging Findings of MIS-C.

Artificial intelligence algorithm can identify the same percentage of women with breast cancer as most radiologists.
Past RBMA President Christie James, American College of Radiology Commission on Economics Chair Greg Nicola, M.D., and Revenue Cycle Coding Strategies President Melody Mulaik discuss the radiology revenue cycle management challenges and solutions of the pandemic.

Ultrasound is an effective follow-up strategy for masses pinpointed with DBT, potentially side-stepping the need for digital mammography and lower radiation exposure.
Imaging volumes fell farther across most modalities in outpatient imaging centers and are taking longer to rebound.
The University of Cincinnati launched a 10-week program that led the department back to roughly 100-percent pre-COVID-19 levels.