







Healthcare reform is game changer but nobody can yet fully articulate the impact of the new rules. How do you plan for the future when there are so many unknowns? This is the second article in a series that examines how healthcare reform is likely to affect radiology practices and how they can prepare for drastic changes to come.
Facility Management
Latest News
Advertisement
Advertisement
Researchers in the radiation oncology department at UCLA’s Jonsson Comprehensive Cancer Center have received a $14 million grant to develop countermeasures that will help treat damage caused by radiological or nuclear threats such as a dirty bomb attack.
Globally, four billion people have no access to imaging services. Several U.S. organizations are part of an effort to share knowledge and resources to bring the benefits of imaging to medical systems in developing nations.
When times get tight, we start to hear complaints about overhead costs and nonphysician staff costs. That’s natural. But don’t let folks jump to conclusions. Just because you don’t know or understand a process doesn’t mean it’s superfluous. When I hear our radiologists mumble “what do all those people do?” I tell them it is time for them to find out. But don’t stick all the work on one person. Use the perceived “crisis” or gripe-fest to educate the staff on processes in the back office.
Musician Sheryl Crow teamed up with the Pink Lotus Breast Center to create the Sheryl Crow Imaging Center, a state-of-the-art breast imaging center based in Los Angeles featuring the latest advancements in digital screening and diagnostic imaging technologies.
“Meaningful use” is on everyone’s mind and sure to be a predominant topic for years to come.
In my last report (Capturing all your money matters. Here’s why) I explained why it matters to capture as much revenue as possible. Let’s recap some of the major reasons for doing this.
Launch of the new fourth-generation network from cellular wireless companies will enable radiologists to upload and download images more than 10 times faster than they have been able to in the past. While wireless mobile applications for imaging are still a distinct minority, the faster speeds could open the door for preliminary reads or image demonstrations on smartphones and iPads.
When hospitals transition from a contract with an independent radiology practice to an in-house model or a multispecialty group, they can expect some growing pains in the form of technological issues and human resources quandaries, as well as general headaches while trying to get the new practice up to speed. Sutter Health in Sacramento, CA, offers an example.
Over the past week I have seen my fair share of our nation’s airports. After seven flights in six days I am ready for landing by land or sea and will not hesitate to don my oxygen mask before assisting my fellow passengers in doing the same.
California radiologists will be required to incorporate radiation dose levels in their reports under a measure signed into law Thursday by Gov. Arnold Schwarzenegger. The measure requires that radiologists include in their reports the dose length product or the CT dose index if the machine is able to calculate it.
Virtual Radiologic announced Sept. 27 it will acquire NightHawk, a publicly traded national teleradiology practice, making Virtual Radiologic the largest radiology practice in the country. However, radiologists aren’t too worried about the deal because Virtual Radiologic still has to compete with thousands of other practices.
After a rapid-fire series of moves, our author finds that Netflix effortlessly follows him everywhere. Too bad it wasn’t the same for images from a patient with a possible thyroid mass.
Now there’s proof after a day of interpreting images radiologists are less accurate, more tired, unable to focus, and experience eyestrain compared to earlier in the day. A study in the Journal of the American College of Radiology compared the ability of radiologists and residents to read bone exams earlier in the day to later in the day.
Three of the most popular MR contrast agents-Magnevist by Bayer Healthcare, Omniscan by GE Healthcare, and Optimark by Covidien-will soon carry labels warning that their use is “inappropriate” for patients with acute kidney injury or chronic severe kidney disease. These and other gadolinium-containing agents will also carry new warnings emphasizing the need to screen patients for kidney dysfunction that puts them at risk for nephrogenic systemic fibrosis, the rare but potentially fatal condition that led the FDA to require warning labels on these agents in 2007.
The biggest player in the imaging center market announced on Monday a technology purchase that will enhance its efficiency as well as expand its reach into the teleradiology field. RadNet also said its acquisition of Image Medical Corporation, the parent of eRAD, for $10.75 million will qualify RadNet for federal stimulus money geared toward adoption of electronic medical records.

The pressure to get faster, more efficient, and more productive is mounting. Healthcare reform, increasing regulations, and declining reimbursements are bearing down.

In recent months we've found a steady and strong interest in the practice-related material we've been presenting on our website.
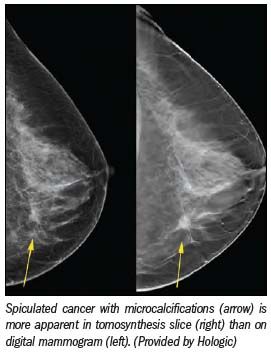
With all the doom and gloom surrounding mammography-lower reimbursement, high threat of malpractice lawsuits-it's easy to assume residents would shy away from the field.
Business consultant Pat Kroken discusses the need to batten down the hatches before provisions of the healthcare reform bill blow in next year. She suggests ways to improve internal billing and collection processes and find lost money.
Before you get on that plane, check the frequent flyers’ round trip special from Rocky Flats Gear: Purchase two pair of men’s radiation-shielding briefs and two pair of women’s briefs and get two pair of bra inserts for free.
A great deal of our time has been spent trying to find ways to make ourselves more efficient. One of those ways we began looking at several years ago was reducing the time we spend in nonbillable activities and in performing procedures that our hospital affiliation requires but that are relatively time-intensive for their reimbursement. To do this, we looked into hiring physician extenders.
A growing body of evidence supports the use of CT colonography for colon cancer screening and a U.S. panel should reverse its decision to not endorse the procedure, according to the CT Colonography Coalition.

Everybody loves to read about the future. We may not be too keen to admit it openly, but we all feel varying degrees of fear and apprehension about what lies around the corner.
CMS codes on radiologic guidance for needle placement is confusing and implementation varies by medical society and payer.
Advertisement
Advertisement
Trending on Diagnostic Imaging
1
Mammography Study Suggests AI Can Bolster the Ability of General Radiologists to Detect Breast Cancer
2
A Closer Look at the Evolution and Emerging Insights with Amyloid and Tau PET for Dementia and Alzheimer’s Disease
3
Could an Emerging Ultrasound Device Facilitate More Efficient Vascular Access Workflows?
4
Study Suggests FDG-PET Better than CT for Assessing Treatment Response for Metastatic Breast Cancer
5